

By Ladd McNamara, M.D.
Everything on this website is for informational purposes only, and not intended as medical advice. Consult your physician before starting nutritional supplements. Please read the full medical disclaimer via the link in the footer below.
Vitamin K2 is the New “Vitamin D,” But Better!
 Are you supplementing with additional vitamin K2 yet? There are significant health benefits to be obtained from vitamin K2, and no known downside. It’s even better if you take vitamin K2 with vitamin D3. Twenty years ago, the news went out how important it is to increase your vitamin D3 intake with supplementation. (Please see my article on this website on “Vitamin D- What Dose Should I Take?”) Now we understand how important it is to also supplement with vitamin K2. Vitamin K2 is the “new Vitamin D,” but better.
Are you supplementing with additional vitamin K2 yet? There are significant health benefits to be obtained from vitamin K2, and no known downside. It’s even better if you take vitamin K2 with vitamin D3. Twenty years ago, the news went out how important it is to increase your vitamin D3 intake with supplementation. (Please see my article on this website on “Vitamin D- What Dose Should I Take?”) Now we understand how important it is to also supplement with vitamin K2. Vitamin K2 is the “new Vitamin D,” but better.
Most people have heard of vitamin K, but may not know the difference between vitamin K1 and K2. These two forms serve quite different functions within our bodies.
Vitamin K1, or phylloquinone, is preferentially used by the liver to activate blood-clotting proteins to allow for coagulation, so you don’t bleed to death from a simple cut on your finger. Vitamin K2, or menaquinone, functions to ensure that calcium is deposited where it should be, such as in your bones, cartilage, and teeth, and not in the soft tissues, such as your arteries, kidneys, and breast tissue. Calcium regulation by vitamin K2 is just as important for preventing your premature death as is appropriate coagulation by vitamin K1.
We get vitamin K1 from green leafy vegetables and nutritional supplements. Although there is vitamin K2 in animal fat, the amount we get from dietary sources is negligible. Most of the vitamin K2 in our bodies is obtained from the endogenous conversion of vitamin K1 to vitamin K2 by our intestinal bacteria and by enzymes within our tissues. (1)
Over the last several years, it has become increasingly apparent that supplementing with additional vitamin K2 has significant health benefits, and that everyone should consider taking generous doses of vitamin K2, along with a daily regimen of broad spectrum quality vitamins, minerals, omega-3 fatty acids, and multiple antioxidants to achieve and maintain optimal health.
The questions are–
- What exactly does vitamin K2 do?
- What form of supplemental vitamin K2 is ideal?
- What dose of vitamin K2 provides optimal results?
- Is taking vitamin K2 safe?
Vitamin K2 Carboxylation – Calcium Binding and Regulation
 Vitamin K2 is the missing link in the calcium supplementation dilemma. You know you need to increase calcium intake for your bones, but too much calcium may increase the risk of cardiovascular disease. However, if you are supplementing with an adequate amount of vitamin K2, any concerns over calcium supplementation are essentially eliminated.
Vitamin K2 is the missing link in the calcium supplementation dilemma. You know you need to increase calcium intake for your bones, but too much calcium may increase the risk of cardiovascular disease. However, if you are supplementing with an adequate amount of vitamin K2, any concerns over calcium supplementation are essentially eliminated.
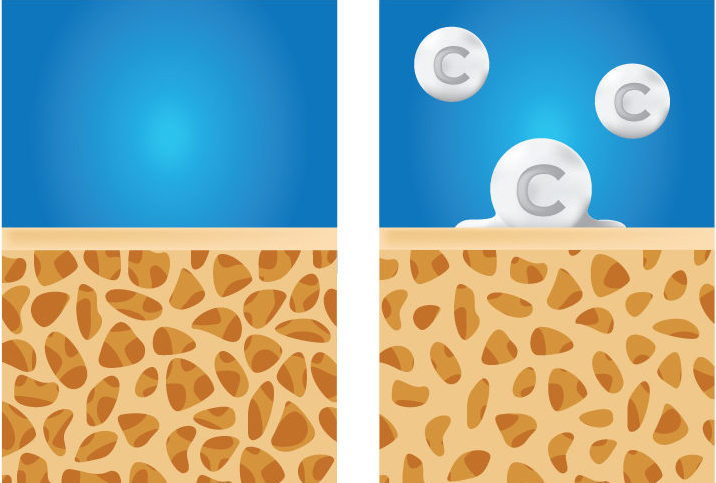
Vitamin K2 helps regulate, or direct calcium in your body, so that you can safely supplement with adequate doses of calcium. Vitamin K2 causes calcium to mineralize into your bones, teeth, and cartilage, where it belongs, and prevents it from mineralizing into your arteries and other soft tissues, thereby reducing the risk of cardiovascular disease. (2)
For the biologically inclined, vitamin K is a cofactor of the enzyme vitamin K carboxylase. In short, vitamin K helps the reaction of carbon dioxide with a protein, giving it a negative charge, and allowing it to bind to a positively charged calcium atom. In this manner, vitamin K2 activates the calcium-binding actions of two proteins — matrix GLA protein and osteocalcin. (3) In the bone, cartilage, and teeth, vitamin K2 binds with osteocalcin, causing osteoblasts (bone cells) to incorporate calcium into those tissues. (4)
In the arteries and other soft tissues, vitamin K2 binds with matrix GLA protein, inhibiting calcium deposition, and causing the removal of excess calcium. (5) Inhibition of calcium deposition in the arteries has huge implications for the reduction of arteriosclerosis, heart disease, high blood pressure, stroke, kidney disease, and more.
Numerous animal studies have shown that vitamin K2 prevents and reverses arterial calcification. (6 – 9) Possible explanations for why human studies have been mixed on showing a reversal of arterial calcification with vitamin K2 include, the low doses of vitamin K2 used in the studies, as well as the short duration of some of these studies (one year or less). Also, the methods of assessment of arterial calcification in humans is limited by imaging techniques, versus in animals the methods of assessment of arterial calcification is performed by dissection and microscopic examination. In other words, small changes can be assessed more easily in animals than humans due to the manner by which they are assessed.
Several human studies are currently underway to assess the reduction of arterial calcification, so I believe we will be hearing additional positive news about vitamin K2 in the near future. (10)
Vitamin K2 Reduces the Risk of Cardiovascular Disease
 In the Rotterdam study, researchers followed men for more than 15 years, and found that those with the highest intakes of vitamin K2 had the lowest risks of severe aortic calcification, cardiovascular disease, and death from cardiovascular disease. (11) It was discovered that the risks of arterial calcification and heart disease were significantly lowered if men were getting at least 32 mcg of vitamin K2 per day.
In the Rotterdam study, researchers followed men for more than 15 years, and found that those with the highest intakes of vitamin K2 had the lowest risks of severe aortic calcification, cardiovascular disease, and death from cardiovascular disease. (11) It was discovered that the risks of arterial calcification and heart disease were significantly lowered if men were getting at least 32 mcg of vitamin K2 per day.
Among postmenopausal women, a time when cardiovascular disease rises due to hardening of the arteries, one clinical study showed that a combination of both vitamin D and vitamin K2 maintained arterial elasticity. (12)
Hypertension and peripheral artery disease are major risk factors of heart disease. Fortunately, an increased intake of vitamin K2 was found to be associated with a decreased risk of peripheral artery disease. (13) Furthermore, the protective effect of vitamin K2 on arteries was particularly pronounced among those with existing hypertension.
Hardening of arteries is due to the building up of plaque over many years. When people think about arterial plaque, most people think of LDL cholesterol. However, arterial plaque consists of 95% calcium, and only 5% cholesterol. Therefore, in order to prevent arterial plaque, that is, to prevent arteriosclerosis, it is reasonable to make our primary focus the prevention of arterial calcification, not the reduction of LDL cholesterol.
If your arteries do not calcify, plaque will not accumulate, and they will not harden, nor will they clog. Without clogged arteries, or arteriosclerosis, you are very unlikely to experience a heart attack or stroke. In addition, without arteriosclerosis, you eliminate the most common cause of chronic kidney disease, end stage renal failure, high blood pressure, and blindness. And if you are a man, without arteriosclerosis, you eliminate the most common cause of erectile dysfunction.
The initiating step of arteriosclerosis development is damage to the endothelium, or lining of the arteries. The endothelium is damaged by free radicals and circulating homocysteine. Homocysteine nicks and damages the endothelium, as well as damages, or more precisely, oxidizes LDL cholesterol.
Oxidized LDL cholesterol sticks within the endothelial nicks. This causes endothelial inflammation, in which white blood cells (macrophages) attempt to gobble up all the oxidized LDL cholesterol, but cannot. The partially “digested” oxidized cholesterol spills out of the macrophages (foam cells) into the arterial wall as a fatty-waxy substance.
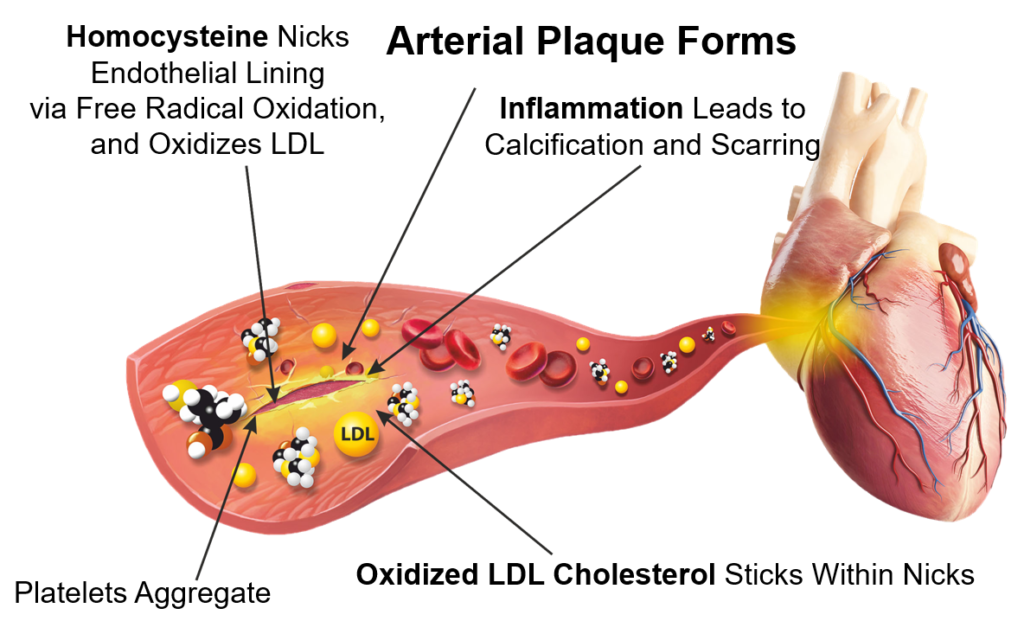
This greasy mess causes even more inflammation, which triggers calcifications, infiltration of smooth muscle cells, and scarring. This pathological process continues on a daily basis over many years, ever thickening the arterial walls with increasing calcifications and scarring bulging into the artery, eventually clogging it. It only takes an arterial spasm, or a sudden increase in cardiac demand for oxygen that cannot be delivered, to cause a heart attack.
The way to prevent heart attacks and arteriosclerosis is to reduce homocysteine levels, protect LDL cholesterol from oxidation, prevent endothelial inflammation, and prevent arterial calcium deposition. All this can be accomplished by eating well, regular exercise, weight control, and daily supplementation with a broad spectrum of quality vitamins, minerals, antioxidants, and omega-3 fatty acids, which includes a generous dose of vitamin K2.
Vitamin K2
- Helps Regulate Calcium Metabolism and Homeostasis
- Helps Protect the Cardiovascular System
- Supports Bone, Cartilage, and Teeth Strength
- May Help Reverse Osteoporosis
- Supports Overall Growth and Development of Fetus, Children, Adolescents
- Improves Hormonal Balance
- May Help Prevent Some Kidney Stones
- May Reduce Risk of Diabetes
- May Inhibit Some Cancers
If you are interested in my specific supplement protocol for prevention of cardiovascular disease, particularly for those with high cholesterol, and/or high homocysteine levels, hypertension, or simply for prevention, please consider a membership in my Dr. Ladd VIP program. Dr. Ladd VIP members have access to all my protocols and much more. You can read more about the benefits of being a Dr. Ladd VIP member by clicking here.
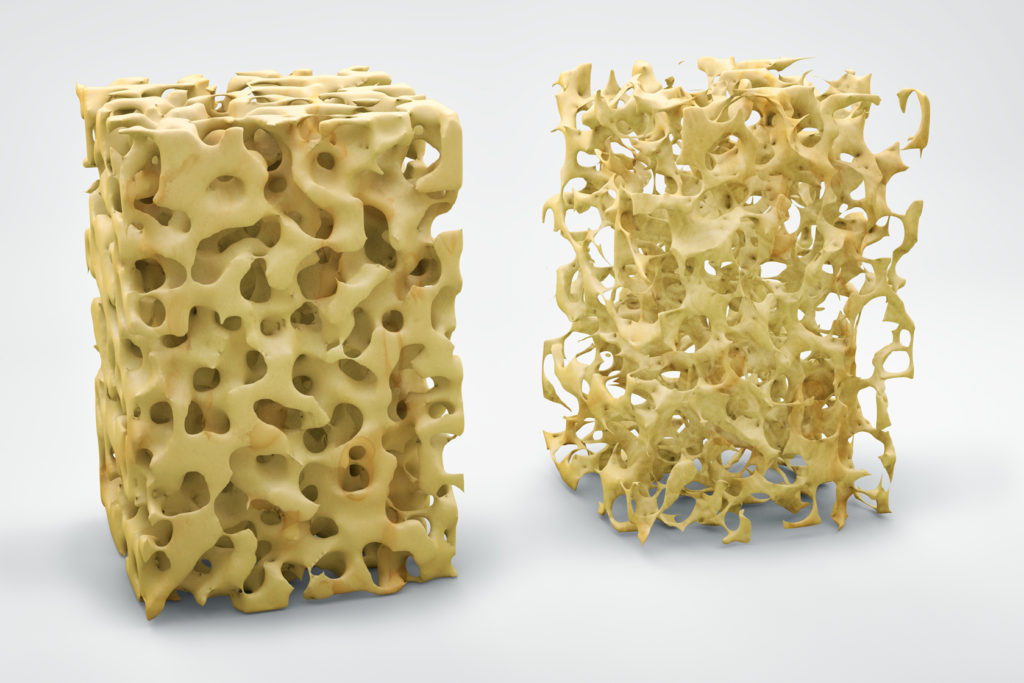
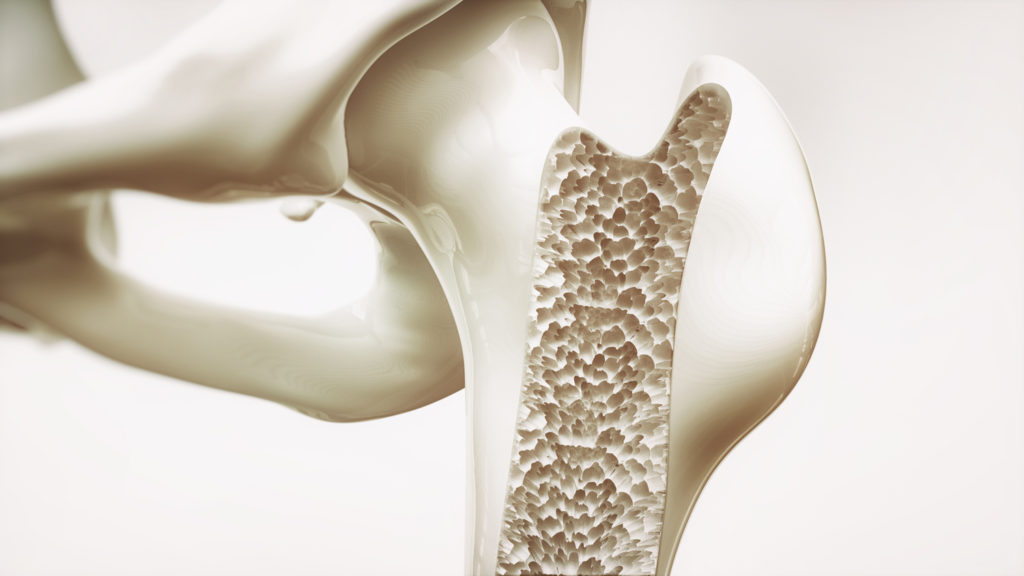
Vitamin K2 Strengthens Bones and May Help Reverse Osteoporosis
 It has long been known that calcium, magnesium, and vitamin D are critical for bone growth, development, and maintenance. It is also now known how critical vitamin K2 is for all these processes.
It has long been known that calcium, magnesium, and vitamin D are critical for bone growth, development, and maintenance. It is also now known how critical vitamin K2 is for all these processes.
During gestation, vitamin K2 is so important that the placenta preferentially transports vitamin K2 over K1 across to the baby to ensure rapid growth and development. (14) After delivery, the mammary glands efficiently convert vitamin K1 into K2, to ensure continued growth and development. (15)
Vitamin K2 supplementation not only helps with growth, development, and maintenance of strong bones, it also helps prevent, and possibly help reverse osteoporosis. (16 – 19) As expected, to reverse osteoporosis a relatively high dose of vitamin K2 is required, compared for use in osteoporosis prevention.
For example, to help prevent osteoporosis, along with supplementing with 800 – 1000 mg of calcium, 400 – 600 mg of magnesium, and 4000 – 6000 IU of vitamin D, a dose of 65 – 180 mcg of vitamin K2 (MK-7) is sufficient. However, to help reverse osteoporosis, in conjunction with the other micronutrients, it appears that a dose of 1,500 mcg per day of vitamin K2 (MK-7) may be required. (If supplementing with the MK-4 form of vitamin K2, it appears that 45,000 mcg per day is required. More on this below.)
Vitamin K2: MK-4 and MK-7 Subtypes
 There are at least eleven different sub-types of vitamin K2, but the two most significant forms for humans are MK-4 and MK-7. (M = menaquinone, K = vitamin K, and the numeral 4 or 7 is for the length of the isoprene molecular chain.) MK-4 is produced by humans and animals, and MK-7 is produced by bacteria.
There are at least eleven different sub-types of vitamin K2, but the two most significant forms for humans are MK-4 and MK-7. (M = menaquinone, K = vitamin K, and the numeral 4 or 7 is for the length of the isoprene molecular chain.) MK-4 is produced by humans and animals, and MK-7 is produced by bacteria.
Both the MK-4 and MK-7 forms of vitamin K2 result in identical beneficial effects in the human body, but there is debate in the health community over which form is best for use in supplements.
Vitamin K2 is found naturally in the body in the MK-4 form, created by conversion from vitamin K1 by both bowel bacteria and enzymes within our tissues. This is the main reason many people might think MK-4 is the desirable form for use in supplements; but, there is much more to know than which form naturally exists within our bodies.
Although MK-4 is found in animal fats, including egg yolk and cheeses, etc., studies have shown there is no appreciable rise in vitamin K2 (MK-4) blood levels from dietary intake or by supplementing with standard doses of MK-4. (More on this below.)
Fermented vegetables, such as natto soy and sauerkraut, provide the MK-7 form of vitamin K2, but unless you are eating these regularly, you would not be getting any MK-7 in your diet. Therefore, the best option to boost vitamin K2 (MK-7) blood levels is via supplementation.
MK-7 stimulates the same biological effects as MK-4. Additionally, MK-7 is converted into MK-4 within the body. So, the question becomes, if we are interested in MK-7 converting into MK-4, why not supplement with MK-4 in the first place, right? The answer—because supplementation with MK-4 does not cause a detectable rise in MK-4 blood levels, and the vitamin K2 effect is gone within hours; whereas MK-7 is much more bioavailable than MK-4, and the effects of MK-7 supplementation lasts for days.
MK-7 is More Bio-Available Than MK-4
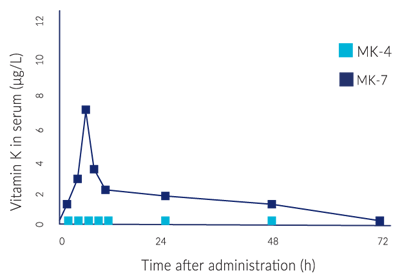 In a study comparing MK-4 and MK-7, subjects were given a single dose of 420 mcg of MK-4 or MK-7. (20) MK-4 was not detectable in the serum of any subject at any point in time. Whereas, MK-7 was well absorbed, and reached maximal serum level at 6 hours after intake. MK-7 was still detectable in the blood up to 48 hours after the initial dose, albeit at low levels.
In a study comparing MK-4 and MK-7, subjects were given a single dose of 420 mcg of MK-4 or MK-7. (20) MK-4 was not detectable in the serum of any subject at any point in time. Whereas, MK-7 was well absorbed, and reached maximal serum level at 6 hours after intake. MK-7 was still detectable in the blood up to 48 hours after the initial dose, albeit at low levels.
The subjects were also given a daily dose of 60 micrograms of MK-4 or MK-7 for seven days. Again, a rise in MK-4 levels was not detectable in any subject throughout the study period. However, 60 mcg of MK-7 significantly increased serum MK-7 levels in all subjects.
This study showed that MK-7 is far more bioavailable than MK-4, and it remains in the serum for a appreciable amount of time. This means that MK-7 provides continuous vitamin K2 beneficial effects to the cells, as MK-7 is converted in the tissues to MK-4 as needed.
Furthermore, studies have shown that a dose of 1,500 mcg per day of MK-4 is required to activate osteocalcin for bone calcium mineralization. (21) In contrast, it only requires 45 mcg per day of MK-7 to activate osteocalcin. These doses are the minimum for maintenance of already healthy bone, not for treatment of osteoporosis.
When treating osteoporosis, a dose of 1,500 mcg per day of MK-7 may be required. In contrast, for the MK-4 form, the Japanese osteoporosis study revealed that 45,000 mcg per day was needed to successfully treat osteoporosis; which is why that dose became the standard recommendation issued by the Japanese Ministry of Health. (22, 23, 24)
As a side note, these studies revealed that long-term high dose vitamin K2 has no toxicity. It is not even known if there is a toxic dose for vitamin K2.
Dose for dose, MK-7 is more effective than MK-4 due to increased bioavailability and a longer half-life compared to MK-4. MK-7 supplementation provides sustained serum levels of vitamin K2. MK-7 creates a virtual “bank,” or reservoir of vitamin K2, in which MK-7 can be continuously converted into MK-4 upon demand.
Based upon both price and effectiveness, MK-7 is a better value than MK-4, which makes MK-7 the ideal choice for use in quality supplements.
Other Possible Benefits of Vitamin K2 Supplementation

As if stimulating the growth, development, and maintenance of healthy bones, as well as to treat osteoporosis and help prevent arteriosclerosis were all not enough reasons to supplement with adequate doses of vitamin K2, there may be additional benefits to this amazing micronutrient. Although not conclusive, there is evidence from human, animal, and laboratory studies that vitamin K2 may help to reduce the risk of diabetes, arthritis, kidney stones, and some cancers. (25 – 30)
Research has shown that various micronutrients help reduce the risk of many chronic diseases. Is it surprising that vitamin K2 would also play a role in supporting optimal health?
In the laboratory, anti-carcinogenic activity of vitamin K2 has been observed in liver, prostate, and breast cancer cell lines. In one study, the effects of varying concentrations of vitamin K2 were assessed on triple-negative and HER2+ breast cancer cell lines. (31) Researchers found a greater cancer inhibitory response with increasing doses of vitamin K2. The inhibitory effects were seen with cell adhesion and proliferation, which resulted in a dramatic reduction in cancer cell growth. Vitamin K2-related compounds were also shown to inhibit cancer cell growth of cells that had become resistant to radiation therapy. (32)
Minimal Vitamin K2 Is Obtained From Most of Our Diets
Although vitamin K2 (MK-4) is found in animal fat, including egg yolk and cheeses, we really don’t get much vitamin K2 from our foods. With no measurable rise in MK-4 from supplementation, you can bet there is no measurable rise in serum MK-4 levels from what most of us eat. Without supplementation, vitamin K2 (MK-4) in our body comes from conversion of vitamin K1, which is obtained from green leafy vegetables.
As mentioned earlier, unless you are eating natto soy regularly, you not getting MK-7 in your diet. This leaves us with supplementation as the most effective means to obtain and maintain consistent vitamin K2 blood levels and benefits.
Some Medications Interfere with Vitamin K2 Status
 Vitamin K1 and K2 are fat-soluble vitamins. Without supplementing with vitamin K2, the only vitamin K2 in your body is derived from conversion of vitamin K1, some of which is converted by your gut bacteria.
Vitamin K1 and K2 are fat-soluble vitamins. Without supplementing with vitamin K2, the only vitamin K2 in your body is derived from conversion of vitamin K1, some of which is converted by your gut bacteria.
Antibiotics kill some of your gut bacteria, and certainly disrupt a healthy bowel microbiome. This can reduce your vitamin K2 balance.
Some medications inhibit, or interfere with fat absorption and metabolism, and can put you at risk for a vitamin K2 deficiency, most notably, the cholesterol-lowering statin drugs. Given that stain drugs are the number one prescribed class of drugs in the world, it is very likely that millions of people are unknowingly suffering a vitamin K2 deficiency, which ironically includes arteriosclerosis.
Medications that put you at risk for a vitamin K2 deficiency include –
- Broad-spectrum antibiotics
- Statins – cholesterol-lowering drugs
- Bile acid medications
- Orlistat – a weight-loss drug (Alli) which reduces absorption of fat-soluble vitamins, including vitamin K1 and K2
Vitamin K2 and Warfarin (Coumadin)
Both vitamin K1 and vitamin K2 supplementation in warfarin therapy is not only safe, but should be considered, as vitamin K use with warfarin usually improves INR control. (33) Warfarin dosage adjustment is almost always required, of course.
 If you are taking warfarin, your doctor may have advised you not to take any vitamins, especially not any with vitamin K (K1). You may have been told to avoid green leafy vegetables, which are high in vitamin K1. However, this is not an absolute rule. In fact, it is considered antiquated advice.
If you are taking warfarin, your doctor may have advised you not to take any vitamins, especially not any with vitamin K (K1). You may have been told to avoid green leafy vegetables, which are high in vitamin K1. However, this is not an absolute rule. In fact, it is considered antiquated advice.
Of course, consult your doctor if you are taking warfarin, but research has shown that people on warfarin who also supplement with a vitamin K-containing multi-vitamin, have more stable INR values than those who do not supplement with vitamin K1. This is because vitamin K1 effectively acts as a counter-balance, preventing wide swings in INR values, reducing the need for frequent warfarin dosage adjustments.
If a person supplements with 150 mcg per day of vitamin K1, their warfarin dose may need to be increased by 15% to maintain the INR value in therapeutic range. It takes a high dose of vitamin K1 (e.g., 700 micrograms per day) to reduce the INR value from 2 to 1.5. (34) But, once the INR value is in therapeutic range, the dosage of warfarin remains quite stable, as long as vitamin K1 and K2 intake remains consistent.
Although vitamin K2 does not affect clotting factors directly, taking high doses of vitamin K2 (MK-7) will affect INR values. For example, a dose of 200 micrograms of vitamin K2 (MK-7) may well lower the INR value from 2.0 to 1.5. This does not mean that if you are taking warfarin that you should avoid vitamin K2, it only means that if you are taking more than 50 mcg of vitamin K2 (MK-7) per day, you need to work with your doctor, and have your INR checked, to know if your warfarin dose needs to be changed. Once you reach equilibrium of the doses of warfarin, vitamin K1, and vitamin K2, which is not difficult to achieve, make sure to be consistent in taking all three.
In addition to achieving a stable INR value, a person on warfarin who supplements with both vitamin K1 and K2 will obtain the many benefits of both these micronutrients. Given the numerous health benefits of vitamin K1 and K2, and the risks of cardiovascular disease and osteoporosis, particularly for those taking warfarin on a long-term basis, it is my opinion that it is far better to supplement with vitamin K1 and K2, and work with your doctor to find the correct warfarin dose for a therapeutic INR, than to go without the benefits of vitamin K1 and K2.
Conclusion
 The health benefits of vitamin K1 and K2 supplementation are clear. And, we will most likely learn of many more benefits in the near future. Vitamin K2 helps incorporate calcium into our bones, cartilage, and teeth, to strengthen these tissues, and helping to reduce osteoporosis, and possibly arthritis. Vitamin K2 also prevents calcium depositing into our arteries, helping to maintain arterial elasticity, and possibly reduce the risk of cardiovascular disease, kidney disease, hypertension, and more.
The health benefits of vitamin K1 and K2 supplementation are clear. And, we will most likely learn of many more benefits in the near future. Vitamin K2 helps incorporate calcium into our bones, cartilage, and teeth, to strengthen these tissues, and helping to reduce osteoporosis, and possibly arthritis. Vitamin K2 also prevents calcium depositing into our arteries, helping to maintain arterial elasticity, and possibly reduce the risk of cardiovascular disease, kidney disease, hypertension, and more.
Vitamin K2 is best supplemented in the MK-7 form, at a dose of at least 180 – 240 micrograms per day to support maintenance of strong bones and elastic arteries. Higher doses (1,500 mcg) of vitamin K2 can safely be taken if attempting to reverse osteoporosis or arteriosclerosis. Of course, vitamin K2 should be supplemented in conjunction with a broad spectrum of quality vitamins, minerals, antioxidants, and omega-3 fatty acids.
Supplementing with only a single micronutrient is never quite enough to achieve and maintain optimal health. All micronutrients work synergistically, and should be taken in proper balance, ratios, and amounts. Knowledge is key, and action is power. Now that you know more, isn’t it time you take control of your health?
Everything on this website is for informational purposes only, and not intended as medical advice. Consult your physician before starting nutritional supplements. Please read the full medical disclaimer via the link in the footer below.
References
- Hirota Y, et al. Menadione (vitamin K3) is a catabolic product of oral phylloquinone (vitamin K1) in the intestine and a circulating precursor of tissue menaquinone-4 (vitamin K2) in rats. J Biol Chem. 2013 Sep 30.
- Maresz K. Proper Calcium Use: Vitamin K2 as a Promoter of Bone and Cardiovascular Health. Integr Med (Encinitas) 2015 Feb; 14(1): 34–39.
- Wen L, et al. Vitamin K‑dependent proteins involved in bone and cardiovascular health (Review). Mol Med Rep. 2018 Jul;18(1):3-15.
- Myneni VD, Mezey E. Regulation of bone remodeling by vitamin K2. Oral Dis. 2017 Nov;23(8):1021-1028.
- Spronk HM, et al. Tissue-specific utilization of menaquinone-4 results in the prevention of arterial calcification in warfarin-treated rats. J Vasc Res. 2003 Nov-Dec;40(6):531-7.
- Wang Z, et al. Vitamin K2 can suppress the expression of Toll-like receptor 2 (TLR2) and TLR4, and inhibit calcification of aortic intima in ApoE-/- mice as well as smooth muscle cells. Vascular. 2018 Feb;26(1):18-26.
- Jiang X, et al. Vitamin K2 regression aortic calcification induced by warfarin via Gas6/Axl survival pathway in rats. Eur J Pharmacol. 2016 Sep 5;786:10-18.
- Ikari Y, et al. Impact of menaquinone-4 supplementation on coronary artery calcification and arterial stiffness: an open label single arm study. Nutr J. 2016 May 12;15(1):53.
- Kurnatowska I, et al. Effect of vitamin K2 on progression of atherosclerosis and vascular calcification in nondialyzed patients with chronic kidney disease stages 3-5. Pol Arch Med Wewn. 2015;125(9):631-40.
- Vossen LM, et al. Menaquinone-7 Supplementation to Reduce Vascular Calcification in Patients with Coronary Artery Disease: Rationale and Study Protocol (VitaK-CAC Trial). Nutrients. 2015 Oct 28;7(11):8905-15.
- Geleijnse JM, et al. Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: the Rotterdam Study. J Nutr. 2004 Nov;134(11):3100-3105.
- Braam LA, et al. Beneficial effects of vitamins D and K on the elastic properties of the vessel wall in postmenopausal women: a follow-up study. Thromb Haemost. 2004;91(2):373–380.
- Vissers LET, et al. The relationship between vitamin K and peripheral arterial disease. Atherosclerosis. 2016 Sep;252:15-20.
- Iioka H, et al. A study on the placental transport mechanism of vitamin K2 (MK-4). Asia Oceania J Obstet Gynaecol. 1992 Mar;18(1):49-55.
- Thijssen HH, et al. Menaquinone-4 in breast milk is derived from dietary phylloquinone. Br J Nutr. 2002 Mar;87(3):219-26.
- Kodama Y, et al. Effectiveness of vitamin K2 on osteoporosis in adults with cerebral palsy. Brain Dev. 2017 Nov;39(10):846-850.
- Rønn SH, et al. Vitamin K2 (menaquinone-7) prevents age-related deterioration of trabecular bone microarchitecture at the tibia in postmenopausal women. Eur J Endocrinol. 2016 Dec;175(6):541-549.
- Huang ZB, et al. Does vitamin K2 play a role in the prevention and treatment of osteoporosis for postmenopausal women: a meta-analysis of randomized controlled trials. Osteoporos Int. 2015 Mar;26(3):1175-86.
- Koitaya N, et al. Low-dose vitamin K2 (MK-4) supplementation for 12 months improves bone metabolism and prevents forearm bone loss in postmenopausal Japanese women. J Bone Miner Metab. 2014 Mar;32(2):142-50.
- Sato T, et al. Comparison of menaquinone-4 and menaquinone-7 bioavailability in healthy women. Nutr J. 2012 Nov 12;11:93.
- Schurgers LJ, et al. Vitamin K-containing dietary supplements: comparison of synthetic vitamin K1 and natto-derived menaquinone-7. Blood. 2007 Apr 15;109(8):3279-83.
- Guralp O, Erel CT. Effects of vitamin K in postmenopausal women: mini review. Maturitas. 2014 Mar;77(3):294-9.
- Hosoi T. [Treatment of primary osteoporosis with vitamin K2]. Clin Calcium. 2007 Nov;17(11):1727-30.
- Shiraki M, et al. Vitamin K2 (menatetrenone) effectively prevents fractures and sustains lumbar bone mineral density in osteoporosis. J Bone Miner Res. 2000 Mar;15(3):515-21.
- Schwalfenberg, GK. Vitamins K1 and K2: The Emerging Group of Vitamins Required for Human Health. J Nutr Metab. 2017; 2017: 6254836.
- Li Y, et al. Effect of vitamin K2 on type 2 diabetes mellitus: A review. Diabetes Res Clin Pract. 2018 Feb;136:39-51.
- Dam V, et al. Association Between Vitamin K and the Metabolic Syndrome: A 10-Year Follow-Up Study in Adults. J Clin Endocrinol Metab. 2015 Jun;100(6):2472-9.
- Yoshida T, et al. Apoptosis induction of vitamin K2 in lung carcinoma cell lines: the possibility of vitamin K2 therapy for lung cancer. Int J Oncol. 2003 Sep;23(3):627-32.
- Xv F, et al. Research progress on the anticancer effects of vitamin K2. Oncol Lett. 2018 Jun;15(6):8926-8934.
- Schwalfenberg GK. Vitamins K1 and K2: The Emerging Group of Vitamins Required for Human Health. J Nutr Metab. 2017;2017:6254836.
- Kiely M, et al. Real-time cell analysis of the inhibitory effect of vitamin K2 on adhesion and proliferation of breast cancer cells. Nutr Res. 2015 Aug;35(8):736-43.
- Amalia H, et al. Vitamin K2-derived compounds induce growth inhibition in radioresistant cancer cells. Kobe J Med Sci. 2010 Sep 28;56(2):E38-49.
- Schwalfenberg, GK. Vitamins K1 and K2: The Emerging Group of Vitamins Required for Human Health. J Nutr Metab. 2017; 2017: 6254836.
- Schurgers L. J., et al. Vitamin K-containing dietary supplements: comparison of synthetic vitamin K1 and natto-derived menaquinone-7. Blood. 2007;109(8):3279–3283.


{kind=link}
thank you, Dr. Ladd, for the detailed explanation of the benefits of K2. I listened to your first program but this article spells the value more clearly. Question: There are so many blood thinners. I have many friends taking other types of blood thinners, not Coumadin. What would you advise in these cases?
Jo, to the best of my knowledge, there are not any conflicts of vitamin K2 or K1 with any other blood thinners (anticoagulants), therefore, taking the vitamin K2 or K1 should not be an issue. Please see the medical disclaimer (link in the footer of this website) about any and all of my statements. Thank you.