
By Ladd McNamara, M.D.
Everything on this website is for informational purposes only, and not intended as medical advice. Consult your physician before starting nutritional supplements. Please read the full medical disclaimer via the link in the footer below.
Introduction
 I had written the bulk of this article a week prior to publishing it here on this website, but due to a combination of my schedule, and a rapidly changing situation, the article is being published a week later than I had hoped. Despite that, and despite being saturated with news about the coronavirus, there is still information to be had, particularly what you can do to reduce your risk of all viral illnesses, and hopefully live with less fear.
I had written the bulk of this article a week prior to publishing it here on this website, but due to a combination of my schedule, and a rapidly changing situation, the article is being published a week later than I had hoped. Despite that, and despite being saturated with news about the coronavirus, there is still information to be had, particularly what you can do to reduce your risk of all viral illnesses, and hopefully live with less fear.
I understand pandemics are scary. However, in my opinion, the mass hysteria surrounding this novel coronavirus, COVID-19, is doing more harm than good. Yes, we need to prepare, and actively take precautions to reduce the risk of serious illness and death form this coronavirus. That is exactly what this article is about, facts, not fear.
I wrote this article mainly to inform you on how to reduce your risk of acquiring and spreading the coronavirus by, mainly by taking precautions, as well as boosting your immune system. We know that those who have low immunity are at risk for this coronavirus. It would then make sense that by boosting your immunity that you may reduce your risk of acquiring this infection. You can boost your immunity with a healthy lifestyle, proper diet, and taking quality nutritional supplements. The research supports this.
Secondly, I wanted to provide information that you may not have heard or read yet, so you can prepare yourself for what’s to come without panicking. I touched on the origin of the coronavirus, as well as the characteristics of the virus, so you know your risks, and what to expect over the next six weeks, and beyond.
Rest assured, this pandemic will end, with the vast majority of people never getting sick; and those who do, will have cold-like symptoms, and will recover and be totally fine. Life will go on.
The questions answered in this article are:
- What is coronavirus, COVID-19?
- What is the origin of COVID-19?
- How Does the COVID-19 Pandemic Compare to Others?
- What are the Complications?
- Who Is Most at Risk of Complications?
- What is the Incubation Period?
- What are The Symptoms?
- How is COVID-19 Contracted?
- How Contagious is it?
- What Should I do If I think I might Have COVID-19?
- What Can We Expect Over the Next Six Weeks?
- What are the Best Precautions to Reduce Risk of Acquiring and Spreading COVID-19?
- What About Travel?
- Dr. Ladd’s Nutritional Supplement Considerations to Support Your Immune System
What is the Coronavirus (COVID-19)?
 Coronaviruses, along with rhinoviruses, are responsible for most upper respiratory infections; i.e., common colds. Coronaviruses are a large family of viruses that can cause symptoms ranging from those of a mild cold to severe pneumonia.
Coronaviruses, along with rhinoviruses, are responsible for most upper respiratory infections; i.e., common colds. Coronaviruses are a large family of viruses that can cause symptoms ranging from those of a mild cold to severe pneumonia.
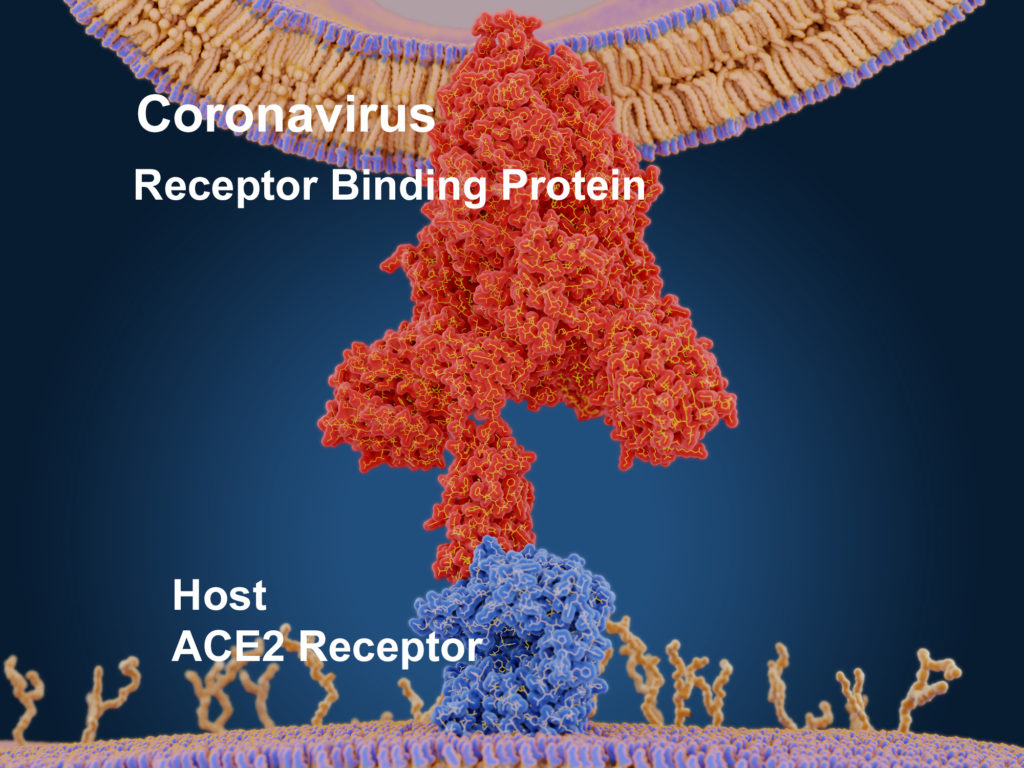
Coronaviruses are so named due to the spikes seen on the shell of the virus, which look like spikes of a crown. (Corona is Latin for crown.) The “spikes” are receptor binding proteins on the shell, which is a phospholipid membrane envelope that encases the viral RNA. The receptor binding proteins allow the virus to attach to specific receptors on host cells.
COVID-19 is so named for Coronavirus Disease 2019, as it was first recognized in December 2019.
COVID-19 was found to be closely genetically related to the SARS coronavirus, particularly the receptor binding protein that caused a pandemic in 2002 – 2003. (1) COVID-19 is so closely genetically similar to SARS, that it is essentially SARS-2, and is now officially named, Severe Acute Respiratory Syndrome Coronavirus 2, or SARS-CoV-2. However, it is commonly referred to as both “the coronavirus” and COVID-19.
Coronaviruses are found in mammals and some birds. They are species specific; for example, to a pig or bat. Coronaviruses are usually only able to infect one species due to very specific binding receptors, but occasionally mutate (or can be bio-engineered in the lab), to be able to “jump” to infect another species, such as humans.
 Coronaviruses only make that jump to humans with close contact with infected animals, or if it is bio-engineered (weaponized) to be able to infect humans, as from a bat coronavirus. At this time, COVID-19 is specific only to humans, and cannot infect your pets.
Coronaviruses only make that jump to humans with close contact with infected animals, or if it is bio-engineered (weaponized) to be able to infect humans, as from a bat coronavirus. At this time, COVID-19 is specific only to humans, and cannot infect your pets.
Although most human coronaviruses cause nothing more than a mild-to-moderate upper respiratory infection (a common cold), and sometimes flu-like symptoms, occasionally, coronaviruses can cause severe respiratory distress, pneumonia, and death, as with the current COVID-19.
Two characteristics to consider about a human coronavirus are infectivity and mortality rate. It can have a high or low infectivity rate (be mildly or highly contagious), and independently have a low or high mortality rate. The current COVID-19 coronavirus has both a high infectivity rate and a moderately-high mortality rate.
However, there is no reason to panic, as most people will not get sick, and those who do, will have nothing more than cold-like symptoms, but because tens of thousands of people will die in the Unites States, and in many other countries, there is every reason to be proactive in taking precautions now! If we are extremely proactive we can mitigate this pandemic, and reduce the number of deaths that will happen otherwise.
What is the Origin of COVID-19?
 For some reason, the powers that be are reluctant to discuss much about the origins of COVID-19. This is perplexing, because in almost all epidemics, let along pandemics, research is always conducted to find the origins of how a virus jumped from animals to humans. The origin of COVID-19 is part of an important story for several reasons. Ultimately, any definite answers about COVID-19’s origins are unsatisfactory, but we do have clues.
For some reason, the powers that be are reluctant to discuss much about the origins of COVID-19. This is perplexing, because in almost all epidemics, let along pandemics, research is always conducted to find the origins of how a virus jumped from animals to humans. The origin of COVID-19 is part of an important story for several reasons. Ultimately, any definite answers about COVID-19’s origins are unsatisfactory, but we do have clues.
Whatever the origin of this coronavirus, it does not change what we are now faced with, and the proactive precautions we need to take. But knowledge is power. Power allows for control in making a difference in our world, and if possible, hopefully preventing future epidemics and pandemics.
I realize that there has always been pandemics, and there will always be pandemics; and that this could have arisen naturally, but there are a few irregularities that raises questions.
What We Do Know
COVID-19 was first discovered in Wuhan, the capital of Central China’s Hubei province, in December 2019. COVID-19 was first thought to have jumped from pangolins, as a whole-genome comparison of COVID-19 found that the pangolin and human coronaviruses share 90.3% of their DNA. However, this was not necessarily suggestive of the origin, because the genetic similarity should be higher (over 95%), before the original host can be identified with confidence.
 Two published studies in February 2020, found the human coronavirus COVID-19 shares 96% of its genome with the bat coronavirus, with the receptor binding protein being identical to that of SARS Cov. (1, 2) This suggests with confidence that the original host is a bat, specifically the Horseshoe Bat.
Two published studies in February 2020, found the human coronavirus COVID-19 shares 96% of its genome with the bat coronavirus, with the receptor binding protein being identical to that of SARS Cov. (1, 2) This suggests with confidence that the original host is a bat, specifically the Horseshoe Bat.
However, there remains a significant mystery surrounding the most important component of infectivity, that of the species-specific receptor binding protein of COVID-19, which allows the coronavirus to attach to human cells (to ACE2 receptors on the epithelial cells of the lungs), — the receptor binding protein of COVID-19 differs from the bat coronavirus! It cannot bind with bat cell receptors. It is identical to that of the original SARS-CoV, which makes one think SARS-CoV2 might be a variant of the original SARS-CoV (as in derived from, but modified). (1)
This tells us that COVID-19 did not directly jump from bats to humans. In other words, COVID-19 came from bats, but cannot infect bats. Therefore, the coronavirus either mutated, and through some unknown intermediary animal host, and somehow lost its ability to infect bats, or more likely it was manipulated (bio-engineered or weaponized) in the lab from the original SARS virus. Is the second option even impossible? Is this a conspiracy theory, or scientific evidence of origin?
Some are calling such considerations a conspiracy theory, and technically, that is true. It is a theory about a possible conspiracy of some sort, such as in being manipulated in the lab or studied in a lab, and then covered up as the pandemic exploded. There are suspicious circumstances, and at minimum, The China Communist Party has not been forthcoming with much needed information since the coronavirus first arose. I will briefly present this controversial issue, without coming to any definite conclusion at this time; but, clearly I am suspicious.
Conspiracy Theory or Suspicious Circumstances?
 Again, COVID-19 may very well have developed naturally, but the strange issue with the loss of the bat receptors on the coronavirus, and some unknown intermediary host species is perplexing. According to the purported report, somehow this virus mutated in an extremely short period of time to not be able to infect bats, and then all of a sudden be able to infect only humans. There are other suggestive statements made by Chinese officials and others that raise suspicions that this virus did not arise naturally.
Again, COVID-19 may very well have developed naturally, but the strange issue with the loss of the bat receptors on the coronavirus, and some unknown intermediary host species is perplexing. According to the purported report, somehow this virus mutated in an extremely short period of time to not be able to infect bats, and then all of a sudden be able to infect only humans. There are other suggestive statements made by Chinese officials and others that raise suspicions that this virus did not arise naturally.
So, let’s look at some facts.
FACT: The first person to contract COVID-19, known as patient zero or the index patient, is unknown. Chinese authorities originally reported that the first coronavirus case was on December 29th, 2019, who supposedly contracted the virus from eating bat soup, which as supposedly acquired from the Huanan Wet Market in Wuhan.
Other than the fact that the Horseshoe bat, which COVID-19 is linked to, does not hibernate in cities in China, and is not sold at the wet market, the supposed index patient, who was an invalid, never set foot in Huanan Wet Market.
FACT: After Chinese citizens in Wuhan circulated information on social media undermining the official story about patient zero and the Huanan Wet Market origin, Chinese authorities revised their statement regarding the index patient and the Huanan Wet Market. The official statement was then changed to be that both the index patient and the origination of the coronavirus were “unknown.”
Many citizens inside Wuhan sacrificed their freedom, and some their lives, to get out vital information about the rapidly-growing epidemic.
UNKNOWN: It was reported on social media by citizens from Wuhan, that the coronavirus escaped from The Wuhan Institute of Virology due to a technician getting infected.
 FACT: In 2015, the Wuhan Institute of Virology opened the first biosafety level 4 (BSL–4) laboratory in mainland China, which is equipped to study virulent deadly viruses.
FACT: In 2015, the Wuhan Institute of Virology opened the first biosafety level 4 (BSL–4) laboratory in mainland China, which is equipped to study virulent deadly viruses.
FACT: Addressing rumors on social media in Wuhan about the origin of the novel coronavirus, the official response from Chinese authorities from the institute was, “The Wuhan Institute of Virology has no infections, and the patient zero did not come from us.”
FACT: Curiously, in mid-February 2020, Chinese leader Xi Jinping spoke about the rapidly-spreading coronavirus in the context of lab safety being a “national security” issue, and the need to protect the people’s health by setting up a national system to control biosecurity risks.
QUESTION: Why speak of the need to increase biosecurity at viral laboratories in the middle of a national viral biohazard emergency, if the coronavirus did not escape from the lab?
FACT: If Xi Jinping’s address was not suggestive enough, the following day, February 21st, the Chinese Ministry of Science and Technology released a new directive titled: “Instructions on strengthening biosecurity management in microbiology labs that handle advanced viruses like the novel coronavirus.” (3)
FACT: Lt. Colonel Dr. Dany Shoham, a former Israeli military intelligence officer who holds a doctorate in microbiology, studied Chinese bio-warfare, and weighed in on the emerging COVID-19 pandemic.
From 1970 to 1991, Dr. Shoham was a senior analyst with Israeli military intelligence for biological and chemical warfare in the Middle East and worldwide. If anyone would have more knowledge about Wuhan Institute of Virology than the average person, it is Lt. Col. Dr. Shoham.
 Dr. Shoham said the Wuhan Institute of Virology is linked to Beijing’s covert biological weapons program.
Dr. Shoham said the Wuhan Institute of Virology is linked to Beijing’s covert biological weapons program.
“Certain laboratories in the institute have probably been engaged, in terms of research and development, in Chinese [biological weapons], at least collaterally, yet not as a principal facility of the Chinese BW alignment,” Mr. Shoham told The Washington Times. (4)
In other words, this suggests that The Wuhan Institute of Virology did not bio-engineer COVID-19, but most likely were reproducing it before it escaped. IF the Wuhan Institute of Virology is involved in a covert bioweapons program, which is highly possible, I do not believe they nor the Chinese Communist Party (government) intentionally released this coronavirus, IF it even escaped from there at all. This does not mean that another group unrelated to China did not release a bioweapon to cause the effects that we are seeing now. (And no, the U.S. military did not release this virus. Not only is there no evidence for that, it is completely absurd.)
FACT: There is “no evidence” that COVID-19 was bio-engineered and/or escaped from The Wuhan Institute of Virology. (However, there are indications that it was bio-engineered.)
FACT: There is “no evidence” that COVID-19 was not bio-engineered, and did not escape from The Wuhan Institute of Virology, or intentionally planted in the wet market.
FACT: COVID-19 did not arise from someone eating bat soup at the Wuhan Wet Market, as is continually being said on TV.
If someone at the wet market was infected, it was an intentional release to unleash a bioweapon on the world. Either way, someone is patient zero, and someone knows what happened.
Bottom Line: Regardless of whether COVID-19 is naturally-occurring or a developed bioweapon from the SARS virus, and accidentally or intentionally released by some covert group (not China and not the U.S. military) to cause the global chaos and to damage the economy, it is ultimately irrelevant to the fact that we are faced with the need to take precautions to protect ourselves from infection, and help slow, and end this coronavirus pandemic.
Ultimately, I think we will discover the truth if this was an intentional release of a bioweapon.
How Does COVID-19 Pandemic Compare to Others?
 As mentioned above, most human coronaviruses cause the common cold, along with rhinoviruses. We have all encountered many coronavirus strains throughout our lives. Many, if not most, of these coronaviruses arise from other mammals. They mutate to be able to infect humans, and then usually only cause minor upper respiratory tract infections.
As mentioned above, most human coronaviruses cause the common cold, along with rhinoviruses. We have all encountered many coronavirus strains throughout our lives. Many, if not most, of these coronaviruses arise from other mammals. They mutate to be able to infect humans, and then usually only cause minor upper respiratory tract infections.
Occasionally, a coronavirus naturally mutates (or is bio-engineered), into a virulent deadly strain that is capable of infecting humans and causing a global pandemic of pneumonia, severe respiratory distress, organ failure, and death. Prior to COVID-19, we experienced this most recently with the SARS pandemic in 2002, and the MERS outbreak in 2012. Unfortunately, the coronavirus outbreak that began in December 2019, is on track to be one of the worst pandemics in the past 100 years. With aggressive precautions we can dramatically mitigate the deaths, and hopefully, the worst part about this pandemic will only be the dramatic non-medical impact on our lives.
Severe Acute Respiratory Syndrome (SARS), 2002. Originated in Southern China from a civet (small nocturnal mammal). Worldwide: 8098 cases, 774 deaths, 9 – 10% mortality rate. In 2004, a smaller outbreak occurred due to contact with the virus in a Chinese virology lab. Moderately contagious, due to the relatively medium load, or number, of viruses needed to infect human cells. No human cases of SARS have been reported anywhere in the world since 2004.
Middle East Respiratory Syndrome (MERS), 2012. Originated in Saudi Arabia from a camel. Worldwide: 2494 cases, 858 deaths, 34 – 35% mortality rate. MERS cases continue to occur, primarily in the Arabian Peninsula. To date, there have been only two confirmed cases of MERS in the US, both in 2014. MERS was not highly contagious as it required a relatively large load of viruses to cause infection.
The number of cases and deaths per year from seasonal influenza fluctuate significantly each year depending upon virulence. For example, in the U.S., the number of deaths per year ranges from 12,000 – 80,000. In Table 1 below, I used the number of ~40,000 deaths from influenza in the United States as an average for the sake of space available in the table.
COVID-19 Compared to 2019 – 2020 Seasonal Flu
As of February 29, 2020, the statistics for the 2019 – 2020 seasonal influenza in the United States were –
- 34 Million Cases
- 350,000 Hospitalizations
- 20,000 Deaths (136 children)
Mortality Rate
 The Mortality Rate of COVID-19 worldwide, that is the number of deaths per cases, is reported by the World Health Organization (WHO) at the time of this writing as 3.4%. However, the mortality rate is only as accurate as the reporting, the accuracy of testing, who is being tested, as well as the availability of critical care, including ventilators.
The Mortality Rate of COVID-19 worldwide, that is the number of deaths per cases, is reported by the World Health Organization (WHO) at the time of this writing as 3.4%. However, the mortality rate is only as accurate as the reporting, the accuracy of testing, who is being tested, as well as the availability of critical care, including ventilators.
In addition, the number of cases reported from China are unreliable, and considered to be much greater than officially reported. With a larger number of nonfatal cases of COVID-19, the denominator becomes larger, and the death rate is calculated to be lower.
South Korea had early access to abundant number of test kits (they created them within South Korea), and to date have tested over 200,000 people. This number FAR surpasses the number of people tested in the United States due to the unavailability of test kits. From early statistics as of March 9, 2020 from South Korea, with 7,869 confirmed cases, with 66 deaths. Calculating 66 deaths out of 7,839 cases equals a 0.8% mortality rate. This number will change as more cases and deaths are reported.(The CDC estimates the mortality rate to be 1.0 – 2.5%.)
Obviously a 1.0 – 2.5% mortality rate is much better than a 3.4%, but it is still 10 to 25 times greater than the death rate of the seasonal flu every year, with an average mortality rate of 0.1%.
The mortality rate among those at greatest risk is much greater than 2.5%. For the elderly over the age of 80, particularly those who are chronically ill, and/or are immuno-compromised, the mortality rate is approximately 15%. For those under the age of 50, at this time the mortality rate for COVID-19 is similar to the seasonal flu, i.e., 0.1%.
Table 1: Comparison of Global Pandemics
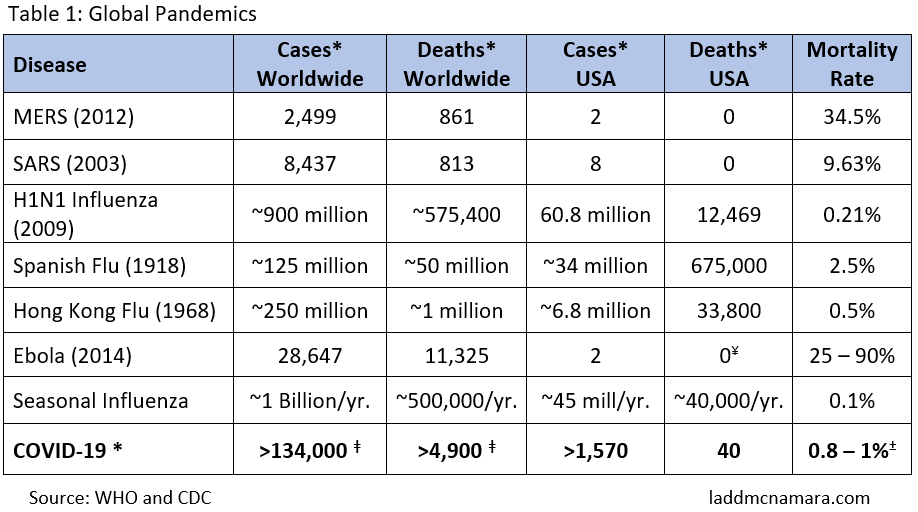
- * Date = March 12, 2020
- ǂ Assuming numbers reported from China are correct, which we truly cannot. The numbers from China are undoubtedly much higher.
- ¥ One person died of Ebola Virus in the United States, but since he contracted it while in West Africa, his death is not counted in the statistics of those who died from contracting the disease in the United States. This patient was treated in Dallas, Texas, where two healthcare workers caring for the patient contracted the disease, and both recovered.
What are the Complications of COVID-19?
 According to the information available from the World Health Organization (WHO) and the Center for Disease Control (CDC) in Atlanta, at the time of this writing, over 85% of people who are infected with the coronavirus will either have mild cold symptoms, moderate flu-like symptoms, or possibly no symptoms at all.
According to the information available from the World Health Organization (WHO) and the Center for Disease Control (CDC) in Atlanta, at the time of this writing, over 85% of people who are infected with the coronavirus will either have mild cold symptoms, moderate flu-like symptoms, or possibly no symptoms at all.
Approximately 15% of people will become seriously ill, and will require hospitalization. One-third of those who become seriously ill, or 5% of the total number of people with COVID-19, will develop pneumonia, respiratory distress, or heart failure. Of those who go into respiratory distress and/or develop heart failure, there is a 50% risk of death (partly dependent upon hospital care).
Although medical care in the United States, and other first-world countries, can provide very good supportive ICU care. However, most ICU units are already running near full capacity, and that poses a problem. What happens when thousands of people, just in the United States, start needing respiratory supportive care in the ICU? Look to the current situation in Italy to get an idea of what we are about to see here (particularly if we don’t take aggressive precautions).
In Italy right now, the situation is dire. Those sick with COVID-19 are overwhelming the hospitals and the ability of the doctors and nurses to provide optimal care, and life and death decisions are being made. In other words, they are deciding who will live and who will die, by deciding who will get the respiratory ICU care, and who will not.
Myth about Pulmonary Fibrosis
There is a myth going around about the coronavirus causing 50% fibrosis of the lungs by the time one has a fever; and then goes on to instruct people to do an inhalation test in the morning to see if you cough. This is a myth. COVID-19 does not cause pulmonary fibrosis.
Many people cough with taking deep breaths when first waking up in the morning, because many lung aveoli have are not fully open, or have a slight amount of fluid in them, due to shallow breathing while sleeping. With deep breaths in the morning you will open up your aveoli and cough out the slight amount of fluid in your lungs. That is one reason why you take deep breaths while bed bound, to avoid bacteria growing in the fluids that build in the lungs from shallow breathing.
Who Is Most at Risk for COVID-19 Complications?
 Anyone of any age can contract COVID-19, but not everyone is equal in the risk of developing complications and death. People over the age of 60, and particularly those with preexisting chronic diseases, such as chronic asthma, COPD, emphysema, chronic bronchitis, heart disease, cancer, and uncontrolled diabetes are at high risk of pneumonia, respiratory distress, and death.
Anyone of any age can contract COVID-19, but not everyone is equal in the risk of developing complications and death. People over the age of 60, and particularly those with preexisting chronic diseases, such as chronic asthma, COPD, emphysema, chronic bronchitis, heart disease, cancer, and uncontrolled diabetes are at high risk of pneumonia, respiratory distress, and death.
Those who are immuno-compromised, as with HIV/AIDS, those who are taking immuno-suppressant medications, or undergoing chemotherapy, are also at high risk of pneumonia, severe acute respiratory distress, heart failure, and death.
As opposed to the average mortality rate of approximately 1%, the mortality rate among those over the age of 80 approaches 15%, due to the presence of other diseases, the inherent weaker immune system that comes with age, or simply poor overall health. This is not to say that if you are younger than 60, and do not have an underlying chronic illness, that you cannot die of COVID-19, but you are far less likely to die than those who are at risk.
ACE Inhibitors and ARB Medications May Put People at Greater Risk of Severe Complications from COVID-19 Infection
Update March 18, 2020: Patients with cardiovascular diseases, hypertension, or diabetes, who are treated with ACE-2-increasing drugs, are at at higher risk for severe complications from COVID-19 infection. As described above, the COVID-19 coronavirus binds to ACE2 (angiotensin converting enzyme 2) receptors that line the epithelial cells of the lungs. ACE2 receptors are also found on the epithelial cells of the intestine, kidney, and blood vessels. This is significant for both the disease process, as well as how medications called, ACE inhibitors can negatively affect the infection.
Angiotensin-converting enzyme inhibitors, or ACE inhibitors and angiotensin II type-I receptor blockers (ARBs), increase the number and activity of ACE2 receptors on the cells. This increases the targets on which the COVID-19 coronavirus binds, theoretically increasing the risk of getting infected, as well as the risk of severe complications once infected.
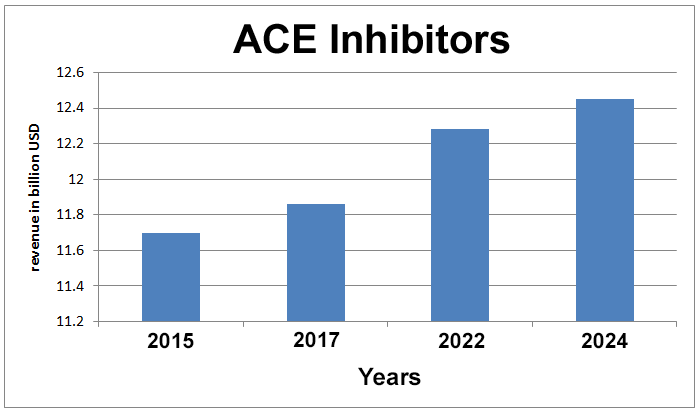
Those with type 1 and type 2 diabetes, high blood pressure, and cardiac disease, are often treated with ACE inhibitors and ARBs. In a recent publication in the medical journal Lancet, it was found that a high percentage of those suffering severe complications and death were taking ACE inhibitors and ARBs. (47) These drugs may not only increase the risk of getting the infection due to increased number of ACE2 receptors on lung epithelial cells, but of great significance, these drugs can trigger cytokine storm; a severe systemic inflammatory process that makes symptoms and complications worse. (Micronutrients, such as beta glucans, modulate, that is, can inhibit cytokine storm. More on this concept at the end of the article.)
Ibuprofen and thiazolidinediones (TZD, also known as glitazones, a class of oral hypoglyemics to treat type 2 diabetes, a common brand name being Avandia) also increase ACE2 receptors throughout the body, including within the lungs. This could help explain why diabetics are in the at-risk group; as well as why those taking ibuprofen when sick with COVID-19 may experience a worsening of symptoms, or even cytokine storm. (47)
Chronic Stress, Lack of Sleep, and Other Conditions Depress the Immune System
Those who are chronically stressed, overworked, under slept, depressed, nutritionally deficient, or consume excess alcohol, will have a weakened immune system, and will also be at increased risk of complications and death from COVID-19. This is why I am emphasizing precautions and taking quality nutritional supplements now! (See below.)
 With seasonal influenza, children under the age of 9 are at risk, similar to the elderly; but fortunately, this is not the case with COVID-19. So far, young children, babies, and even babies born to women sick with COVID-19 are not getting seriously sick. However, they remain susceptible to seasonal influenza, currently in process. And the precautions I am giving here, including supplementation, will help protect children from serious illness from the flu.
With seasonal influenza, children under the age of 9 are at risk, similar to the elderly; but fortunately, this is not the case with COVID-19. So far, young children, babies, and even babies born to women sick with COVID-19 are not getting seriously sick. However, they remain susceptible to seasonal influenza, currently in process. And the precautions I am giving here, including supplementation, will help protect children from serious illness from the flu.
Pregnant women tend to have reduced immunity, and are at increased risk of seasonal influenza, and tend to get sicker than non-pregnant women when they catch a cold or flu.
Fortunately, most of us will either not get COVID-19, or only have mild-to-moderate cold symptoms. However, all of us should take active measure to strengthen our immune systems, and reduce the spread of the virus to others, particularly to protect the deaths of those most vulnerable.
What is the Incubation Period of COVID-19?
Although there have been a few reports of people becoming ill with COVID-19 after 21 days of exposure to a contagious person, the accepted incubation period of COVID-19 is currently thought to be 2 – 14 days, with an average of 5 days from contracting the virus to expression of symptoms.
However, one becomes contagious within 24 to 48 hours after contracting the virus, long before symptoms ever occur, and IF they even occur. This means that we ALL must take active precautions to avoid contracting and spreading the virus to others if we are going to shorten the course of this pandemic and mitigate the number of deaths.
What are The Symptoms of COVID-19?
 It is important to recognize the symptoms of COVID-19, and contact your doctor or health department if you have symptoms, particularly if you have a high spiking fever, a persistent cough, and shortness of breath. Elderly people tend to not spike high temperatures when ill. A temperature of 99.6 F (37.5 C) is enough to indicate COVID-19 infection in those 65 years old and older. Now that more test kits will be available in the United States, more people can finally be tested to confirm suspected cases.
It is important to recognize the symptoms of COVID-19, and contact your doctor or health department if you have symptoms, particularly if you have a high spiking fever, a persistent cough, and shortness of breath. Elderly people tend to not spike high temperatures when ill. A temperature of 99.6 F (37.5 C) is enough to indicate COVID-19 infection in those 65 years old and older. Now that more test kits will be available in the United States, more people can finally be tested to confirm suspected cases.
If you have been exposed to COVID-19 (and soon tens of millions of people will be), and if you experience symptoms of COVID-19, and particularly if you are in the “at-risk” population (see above), be sure to call your doctor or health department before going in and infecting others. Of course, if you are having respiratory distress, i.e., difficulty breathing, then obviously, this is an emergency, and it is time to call 911.
Remember, you could be contagious without having symptoms, as well as contract the virus from others who are asymptomatic.
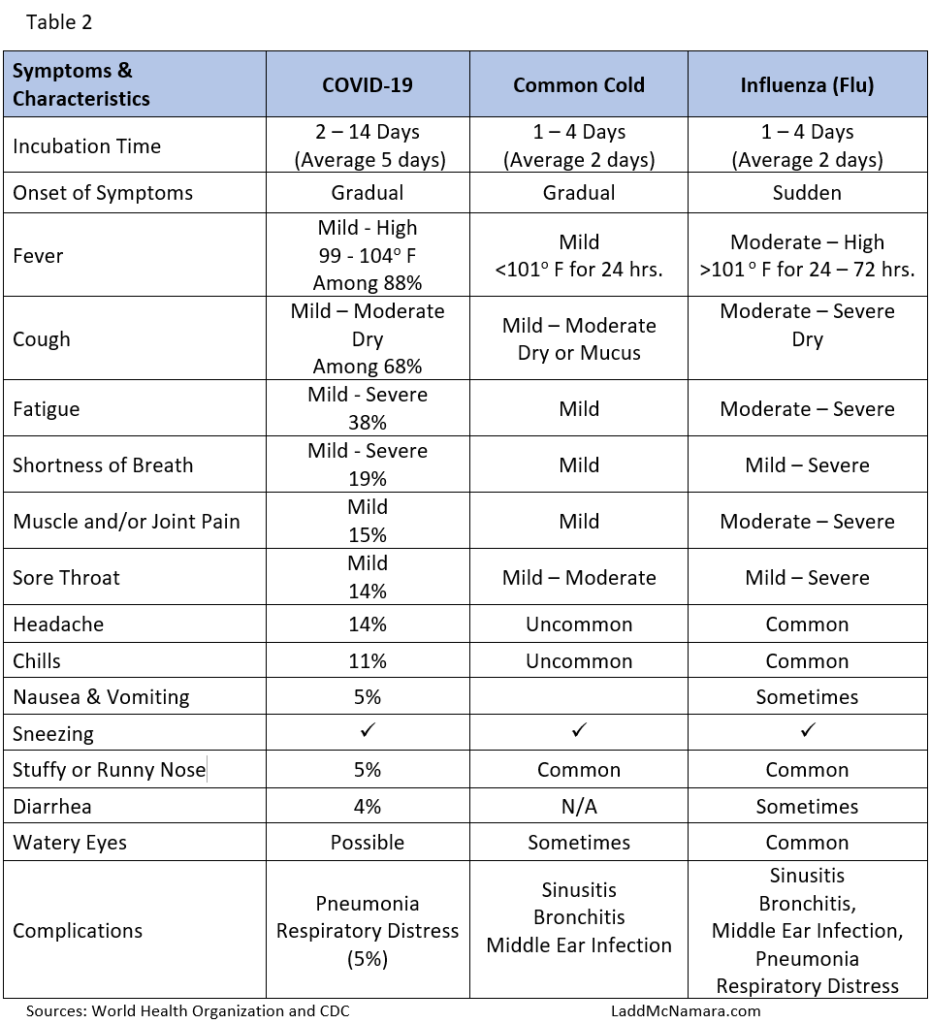
Although nonspecific, the most common symptoms of COVID-19 are those of a common cold, except the fever is often higher than with a cold. Eighty-eight percent of those who get sick with COVID-19 have fever, and 68% have dry cough, and 19% experience shortness of breath.
Common Symptoms of COVID-19
- Fever (88%)
- Dry Cough (68%)
- Fatigue (38%)
- Mucus (sputum production) (33%)
- Shortness of Breath (19%)
Other symptoms of the common cold are also reported, as well as a smattering of reports of gastro-intestinal upset and diarrhea. Table 2 shows the symptoms and characteristics of COVID-19 compared to the common cold (upper respiratory infection) and the seasonal flu (influenza).
How is COVID-19 Contracted?
There are two ways of contracting the COVID-19 infection, inhaling of aerosolized contaminated saliva micro droplets (airborne), and self-inoculation by touching your face after touching a COVID-19-contaminated surface (contact).
Airborne
 COVID-19 coronavirus is transmitted via viral-laded respiratory droplets that are expelled from an infected person’s lungs with speaking, laughing, coughing, or sneezing. The closer in proximity to a contagious person, the increased likelihood of inhaling a greater number of contaminated saliva micro droplets.
COVID-19 coronavirus is transmitted via viral-laded respiratory droplets that are expelled from an infected person’s lungs with speaking, laughing, coughing, or sneezing. The closer in proximity to a contagious person, the increased likelihood of inhaling a greater number of contaminated saliva micro droplets.
According to researchers from M.I.T. who studied the pattern of droplets spewed into the air from our lungs, one cough produces 3000 droplets, the same as talking for 5 minutes. A single sneeze produces 40,000 droplets of various sizes. (5) Larger droplets fall to the ground within 6 – 8 feet, and can contaminate all surfaces upon which they land. However, micro droplets travel much further, a minimum of 15 – 20 feet.
Of concern with highly infectious bacteria and viruses such as COVID-19, is that very small micro droplets, whether produced from coughing, sneezing, heavy breathing, or talking, can remain airborne for up to 3 hours, if not indefinitely under certain conditions (cool air temperature and high humidity).
The micro droplets become more dilute the further they spread from the source. With most other viruses, staying 3 feet away from others is usually enough to reduce the risk of infection, as it usually takes quite a number of viruses to take seed in your lungs. This is not the case with COVID-19. The micro droplets can be quite dilute in the air, and when inhaled, they can still cause an infection, which makes this coronavirus quite infectious. Keeping a distance of at least 6 feet is required to minimize infection.
Yes, one virus that enters your lung cells can cause infection, but it takes exposure to more than one to get sick.
It only takes one sperm to get pregnant, but in reality it takes tens of millions of sperm, all traveling together to make it through the barriers to reach the egg, all so that one sperm can fertilize it. With an airborne viral infection, it takes many viruses to make it past the barriers of your mucous membranes and immune system. How many viruses depends upon how infectious it is, which is discussed below.
 Certainly, confined areas will retain a higher concentration of contaminated micro saliva droplets, which will increase the risk of getting infected, than being in open spaces.
Certainly, confined areas will retain a higher concentration of contaminated micro saliva droplets, which will increase the risk of getting infected, than being in open spaces.
On March 9, 2020, The South China Morning Post reported on a study published in the peer-review journal Practical Preventive Medicine on March 6, 2020 (now removed from the journal for unknown reasons) illustrating the airborne contagious nature of this virus. (6)
Through CCTV, in January 2020, researchers were able to follow the route of a sick man sitting on the back of a bus who was diagnosed with COVID-19. They were able to determine that he infected passengers 6 rows in front of him (4.5 meters, or roughly 15 feet). In addition, people contracted the coronavirus infection 30 minutes after he left the bus. Of note, no passengers wearing masks while he was on the bus contracted COVID-19.
The Coronavirus Can Remain Active in the Air within Saliva Micro Droplets for 3 Hours or More
From this study, and from the M.I.T. study on saliva droplets, it is clear that salvia micro droplets can carry viral particles for long distances since they remain airborne up to 3 hours. Even remaining airborne for 10 to 30 minutes is clearly enough time to remain concentrated enough in a confined area to cause transmission and infection of other people, long after the contagious person may have left the area.
Saliva micro droplets can be taken up in ventilation intakes, and spread through air ducts anywhere in a building. Theoretically, without a high quality HEPA filter, as found in most hospitals and airplanes, the coronavirus can be spread about into other rooms, IF it gets into the intake vents.
 Crowds and confined spaces, such as rooms, buses, trains, subways, cruise ships, and airplanes are all confined, crowded spaces, that place people in close contact.
Crowds and confined spaces, such as rooms, buses, trains, subways, cruise ships, and airplanes are all confined, crowded spaces, that place people in close contact.
The waiting rooms of doctor’s offices and hospitals are not only crowded and confined, it is where you are most likely going to encounter a sick person. If you are over the age of 60, and especially have an underlying chronic disease, or of any age and are at-risk, if you must travel or be in a crowded confined space, it is very wise to wear the a proper N95 or N99 mask (see below on precautions).
As mentioned, most hospitals and airplanes have the proper HEPA filtration which can filter out viruses from the ventilation system. Not all HEPA filters are created equally, so if you have a HEPA filter for your home or small business, make sure your HEPA filter is certified to filter viruses and mold. In addition, some areas in hospitals (such as the entrance to the OR) are equipped with UVC (ultra violet C) lights, which rapidly kill bacteria and viruses.
Far UV Light Could Be the Answer to Stop Future Pandemics and The Flu
Decades ago, it was discovered that UVC light, which has a wavelength between 200 – 400 nm, is effective at killing bacteria and viruses by quickly destroying the bonds that hold DNA and RNA together. However, UVC light can also cause skin damage, skin cancer, and cataracts. Since most people do not stand in front of UVC lights at hospitals or in laboratories, but are either shielded or quickly walk by, there is essentially no harm.
 UVA light, used in black lights, does not kill bacteria and viruses, neither does UVB light, used in tanning beds. However, UVB light can cause skin damage and skin cancer with repetitive and prolonged exposure (tanning).
UVA light, used in black lights, does not kill bacteria and viruses, neither does UVB light, used in tanning beds. However, UVB light can cause skin damage and skin cancer with repetitive and prolonged exposure (tanning).
UVA, UVB, and UVC light all emitted from the sun, along with visible light, but UVC light is filtered out by the ozone layer, so essentially none of it makes it to the ground to cause harm.
Interesting for future application, researchers at the Center for Radiological Research at Columbia University Irving Medical Center (New York), found that low doses of “far-ultraviolet C” or far UVC light (207–222 nm) can kill airborne viruses within seconds, as well as bacteria and viruses on surfaces where the light can shine, without any causing any skin or eye damage.
Far UVC light is also emitted from the sun, but it does not penetrate the atmosphere, but hits oxygen molecules (O2), splits them apart, and allows them to combine together as O3, or ozone. In summary, far UVC light creates the ozone layer, and in turn, the ozone filters out harmful UVC light.
Here on earth, we can only get far UVC light through special far UV light bulbs. Far UV light is safe and kills viruses and bacteria. Although far UV light bulbs are costly, if mass produced, far UV light bulbs could be economical enough to be placed in all public areas, such as airports, office buildings, stadiums, doctor’s offices, malls, grocery stores, restaurants, schools, churches, virtually anywhere people gather. Far UV light very likely could be the answer to greatly reduce the spread of all future pandemics, as well as greatly reduce the number of deaths from tuberculosis and the seasonal flu. (10)
Self-Inoculation
 In addition to inhaling contaminated saliva droplets, you can inoculate yourself by touching your face after touching a contaminated surface. The coronavirus does not enter through your skin, but through the mucous membranes of your mouth, nose, and eyes.
In addition to inhaling contaminated saliva droplets, you can inoculate yourself by touching your face after touching a contaminated surface. The coronavirus does not enter through your skin, but through the mucous membranes of your mouth, nose, and eyes.
Surfaces become contaminated with coronavirus both by saliva droplets landing on surfaces and by infected people touching literally anything. One can pick up the virus from any surface – metal, glass, plastic, fabric, or paper.
Think about what you and others touch on a daily basis, and then think of an infected person touching these same surfaces. If it helps you to be more cautious, think of people with feces on their hands touching the surface just prior to you touching it, as that is not far off, as many people do not wash their hands, even after bowel movements. (Do not be one of them!)
Stop Shaking Hands
Consider the hands of people contaminated with the coronavirus, the influenza virus, and fecal bacteria every time you reach out to touch a doorknob, door handle, faucet, toilet flush lever, shopping cart, ATM, store keypad, communal pen for signing a receipt, computer keypad, glass screen, gas pump handle, handrail, bus strap or bar, counter top, table, chair, the back of your seat and arm rests on an airplane, your tray on the airplane, towel, purse, money, etc.
 Of course, you can go directly to the contaminated source, and shake the hands of others. If the contagious person does not cough or sneeze on you, he or she may have coughed in his or her hand recently, not washed it, and then extend his or her hand to you. AND, even if that person is not sick with COVID-19, what if he recently touched a contaminated surface?
Of course, you can go directly to the contaminated source, and shake the hands of others. If the contagious person does not cough or sneeze on you, he or she may have coughed in his or her hand recently, not washed it, and then extend his or her hand to you. AND, even if that person is not sick with COVID-19, what if he recently touched a contaminated surface?
Everyone’s hands are always getting contaminated with bacteria and viruses, most of which will not cause illness. However, self-inoculation with contaminated hands to your face is one of two main (if not the main) route of transmission for both COVID-19, the common cold, and the seasonal flu. And, all it takes to significantly reduce the chance of getting sick is to wash your hands with warm water and soap for 20 – 30 seconds before touching your face.
Whether breathing in aerosolized viral-laden saliva micro droplets, or inoculating yourself by touching your face, the viruses make their way into your lungs, where they attach to your cells and inject their RNA genetic material, which hijack your cells’ DNA and cause it to produce more viruses.
The Circulating Myth About the Coronavirus First Infecting Your Throat
There is another myth about COVID-19 first infecting your throat, and if you swallow hot tea or water you can prevent infection. Although there is some truth to swallowing liquids frequently to swallow viruses that land in your in your throat before they are inhaled into your lungs, but this would not be a major way to prevent infection.
The coronavirus does not infect your throat. The COVID-19 coronavirus has receptor binding proteins for ACE2 receptors that line the eptihelial cells of your lungs. It does not infect cells within the throat. You would only be lucky to swallow all the viruses each time you were exposed before they made it to your lungs, but this will not stop the viruses that remain airborne all the way deep into your lungs. Although theoretically mildly helpful to frequently swallowing water, this method of prevention would only have a small effect on helping to prevent infection.
Question: Does the Flu Vaccine Protect You from COVID-19
No, the flu vaccine does not protect you from COVID-19. Flu vaccines are created against influenza viruses, which are completely different than the coronavirus and rhinovirus families. In addition, the flu vaccine is only 45 – 50% effective anyway. Studies have shown that those with the highest blood levels of vitamin D, have less risk of getting the flu than those who get the flu vaccine. (See below in the Supplement Section).
Question: Can You Get the Flu and COVID-19 at the Same Time?
Yes, it is possible, as the coronavirus and COVID-19 are two different types of viruses. Although it is statistically unlikely to get both at the same time, it is possible.
How Long Does the Coronavirus Remain Active on Surfaces?
 Whether a surface looks clean or dirty is irrelevant, it is usually contaminated with several strains of viruses and bacteria. Complied information from 22 studies on coronaviruses (focusing on SARS and MERS), allows us to know the duration that COVID-19 may remain active on various surfaces. (7) Cold temperatures and/or humid conditions allow the viruses to remain viable longer than in hot and/or dry climates.
Whether a surface looks clean or dirty is irrelevant, it is usually contaminated with several strains of viruses and bacteria. Complied information from 22 studies on coronaviruses (focusing on SARS and MERS), allows us to know the duration that COVID-19 may remain active on various surfaces. (7) Cold temperatures and/or humid conditions allow the viruses to remain viable longer than in hot and/or dry climates.
At room temperature, coronaviruses can remain viable on hard surfaces, such as metal, glass, and plastic for up to 9 days, and on fabric or paper for up to 3 – 4 days. (7) Under very specific circumstances, that of cold and wet conditions, nonhuman coronaviruses have been documented to remain viable for as long as 28 days. This does not mean that COVID-19 is capable of the same, however assume that this novel coronavirus is viable on surfaces for at least 4 to 5 days.
“Human coronaviruses can remain infectious on inanimate surfaces at room temperature for up to 9 days. At a temperature of 30°C [86°F] or more, the duration of persistence is shorter. Veterinary coronaviruses have been shown to persist even longer, for 28 days.” (7)
Transmission via fecal material may also be a route of transmission, but this is not confirmed. You come in contact with fecal material by touching objects, such as money, and shaking hands of people who do not thoroughly wash their hands.
Polls show that between 30 – 40% of people do not always wash their hands after using the bathroom, and that includes following a bowel movement as mentioned above. And, of those who do wash their hands, half of those, do not use soap. I discuss washing your hands properly in the precautions section below.
If you thoroughly wash your hands (with soap, of course), after touching any public surface, along with daily sani-wiping commonly touched surfaces, you would reduce your risk of contracting COVID-19, as well as colds and the flu. If you are in the at-risk population (underlying health condition and/or elderly), and you combine frequent handwashing before touching your face, and wore a proper mask (see below) in crowded, confined spaces, you would significantly reduce your risk of contracting the coronavirus, as well as seasonal influenza, which kills tens of thousands of people (including children), every year in the United States.
How Contagious is COVID-19?
 How contagious is COVID-19? The short answer is very! COVID-19 is more infectious than coronaviruses and rhinoviruses that cause the common cold, as well as viruses that cause the seasonal flu. COVID-19 is about 20 TIMES MORE contagious than the original SARS (2002).
How contagious is COVID-19? The short answer is very! COVID-19 is more infectious than coronaviruses and rhinoviruses that cause the common cold, as well as viruses that cause the seasonal flu. COVID-19 is about 20 TIMES MORE contagious than the original SARS (2002).
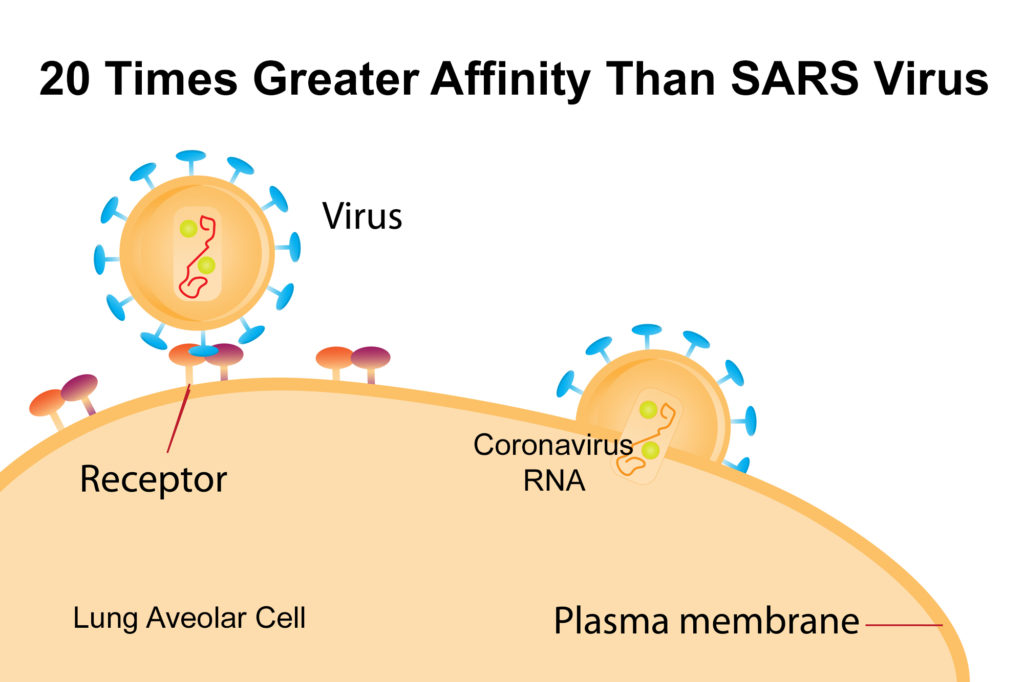
SARS and COVID-19 coronaviruses have specific receptor binding proteins, those are the spikes of the “crown” of coronaviruses, that bind to specific receptors on the lung aveolar epithelial cells. With COVID-19, the receptor binding proteins bind to angiotensin-converting enzyme 2 (ACE2) receptors on the cell surfaces of aveolar epithelial cells within the lungs.
COVID-19 is more contagious, or infectious, than these other viruses because this coronavirus has a greater affinity to these cell receptors. In fact, COVID-19 binds with a 20 times greater affinity to the ACE2 receptors than that of the SARS coronavirus of 2002. (8) This means it takes 20 times fewer COVID-19 viruses to infect your lung cells. Which theoretically means, it is 20 times easier to get infected with COVID-19 than it was with SARS, and the same could probably be said for most other coronaviruses that cause colds, as well as most flu viruses.
The Reproduction Number — R0
In the 2011 movie “Contagion,” starring Matt Damon, a bat-to-pig, and then to human coronavirus pandemic arose out of Hong Kong, and led to a worldwide highly contagious, and fatal pandemic. We are not seeing the level of fatality with COVID-19 as depicted in the movie, but I bring this up because, if you saw the movie you were introduced to the term R0 (“R naught”, where “naught” means a zero, or a number). Epidemiologists use the term R0 (R naught), or “Reproduction Number,” to estimate the number of individuals that an infected person will infect.
 The R0 depends upon various factors, which includes the viral characteristics (such as binding affinity, stability in the environment, incubation period, transmission route, etc.), as well as factors of the population, such as population density, closed or open environment, climate, etc. For example, a contagious person is more likely to transmit the virus to others on a crowded bus or subway car than on a hot day at the beach. Assuming all things being equal with how people function in society, we can compare the Reproduction Number, or R0 of various pandemics to get an idea of the infectivity of a pathogen.
The R0 depends upon various factors, which includes the viral characteristics (such as binding affinity, stability in the environment, incubation period, transmission route, etc.), as well as factors of the population, such as population density, closed or open environment, climate, etc. For example, a contagious person is more likely to transmit the virus to others on a crowded bus or subway car than on a hot day at the beach. Assuming all things being equal with how people function in society, we can compare the Reproduction Number, or R0 of various pandemics to get an idea of the infectivity of a pathogen.
Table 3 below lists several pandemics, with their reproduction number (R0), in which an R0 of 1, means that an infected person is likely to infect one other person in the population. An R0 of 2, obviously means the person will infect two other people, and so on. It may not sound like a big difference, but with each increase in number, there is a huge logarithmic growth rate with each generation as it progresses.
Even an R0 of 2 is quite significant. For example, for a fun exercise, figure out the amount of money you would have if you could double the amount of a penny every day for 30 days. I will get you started. On day one, you would have 1 cent. On day two, you would have 2 cents. Day three, 4 cents. Day four, you would have 8 cents. On day five, 16 cents, and so on. If you have not done this exercise before, please take the time to figure it out, as you will be astounded at how much money you would have on day 30. This is to illustrate the power of logarithmic growth of an R0 of 2. Imagine the significance of an R0 of 3 or more!
According to the World Health Organization (WHO), the reproduction number (R0), also known as “secondary infections,” of COVID-19 as of March 2020 is currently calculated to be between 2.0 and 2.5. However, according to WHO, estimates for both COVID-19 (and influenza viruses) are context and time-specific, making direct comparisons difficult. This means, it is difficult to compare the R0 due to the differences in population density of various societies and communities, cultural customs, as well as variables in local climate and seasonal conditions, and several other factors. However, given how a disease spreads within communities of various population densities, the overall comparisons of R0 values give us a relative indicator of how contagious a pathogen is, and allows for a prediction of how it will spread in the population if unchecked.
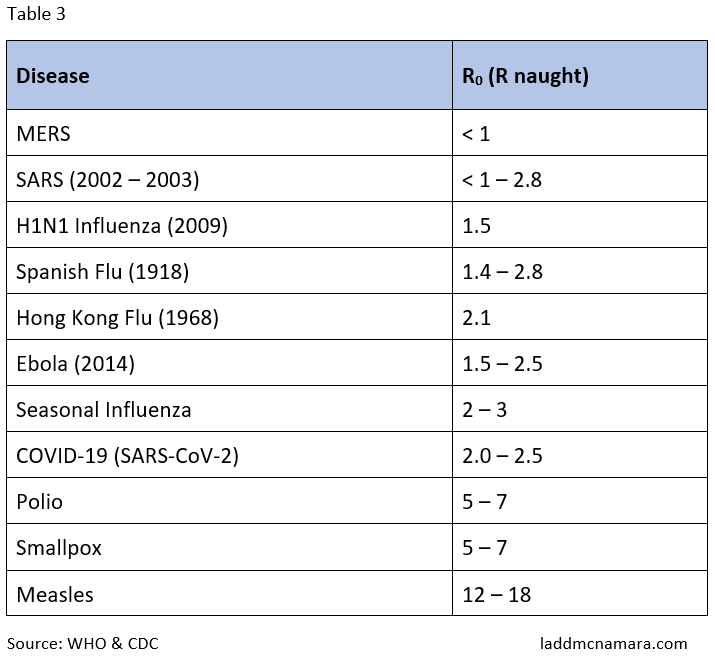
As you can see from this table, COVID-19 is more infectious than the seasonal influenza virus, but not as infectious as the most contagious viral disease, measles, with an R0 of 12 – 18. However, with an R0 of 2 to 2.5 you can expect it to come to your community very soon. The good news, most people will not get sick, and most people who do, will not have more than a common cold.
What Should I do If I think I might Have COVID-19?
 If you do NOT have symptoms, you do not need to be tested. If you have symptoms of COVID-19, and especially a spiking high fever and cough, now that COVID-19 is here, it would be best to be tested now that widespread testing will be available. Older people do not spike high fevers as younger people. People over the age of 65, who have a fever of 99.6 F or higher, who have a cough, and/or shortness of breath should be tested.
If you do NOT have symptoms, you do not need to be tested. If you have symptoms of COVID-19, and especially a spiking high fever and cough, now that COVID-19 is here, it would be best to be tested now that widespread testing will be available. Older people do not spike high fevers as younger people. People over the age of 65, who have a fever of 99.6 F or higher, who have a cough, and/or shortness of breath should be tested.
Remember, it is cold and flu season as well, so most cold symptoms will be the common cold, and most flu-like symptoms will be the flu. However, the flu is still concerning. If you are unsure as to whether you should be tested, call your doctor or health department, and let them know your concerns and symptoms. They can instruct you further.
There will soon be drive-thru testing stations in the parking lots of Walmart, CVS, Walgreens, Target, and others, for those with symptoms of COVID-19. Beware of bogus online test kits. Customs and Border Patrol recently seized thousands of counterfeit at-home test kits. If effective at-home test kits are sold online, make sure they are recommended by official sources first, by checking the official website (e.g., the CDC, or Department of Health). For now, I recommend only being tested at official testing facilities. Again, if you do not have symptoms, you do not need to be tested.
If you get sick with symptoms of COVID-19, do NOT go to the emergency room (unless you are having trouble breathing of course), and do not go to your doctor’s office or health department without calling first (unless instructed otherwise). As with any cold, there is no cure for coronavirus, and almost all who become sick with COVID-19 will be able to recover at home in self-isolation. As with all other colds and flu, you recover at home with plenty of fluids, use only acetaminophen as necessary (NOT other NSAIDs), and highly consider taking quality nutritional supplements (see below).
Questions About Use of Ibuprofen with COVID-19
 Update March 19, 2020: On March 17, 2020, The World Health Organization originally cautioned against taking ibuprofen to manage symptoms of COVID-19. The concern stemmed in part from remarks attributed to an infectious disease doctor in France. She reported to have cited four cases of young patients with COVID-19 with no underlying health problems who went on to develop serious symptoms after using ibuprofen in the early stage of symptoms. (48)
Update March 19, 2020: On March 17, 2020, The World Health Organization originally cautioned against taking ibuprofen to manage symptoms of COVID-19. The concern stemmed in part from remarks attributed to an infectious disease doctor in France. She reported to have cited four cases of young patients with COVID-19 with no underlying health problems who went on to develop serious symptoms after using ibuprofen in the early stage of symptoms. (48)
However, for those not already prescribed ibuprofen, if experiences COVID-19 symptoms, there are over-the-counter alternative analgesics to ibuprofen. It is my opinion that if a person is experiencing fever and body aches, it would be prudent to take acetaminophen (which is the same generic medicine as paracetamol), rather than ibuprofen. Why risk it when you have an alternative?
Be Responsible – Self-Isolate When You are Sick
 Above all, do NOT expose other people to the virus if you are sick with any contagious illness (cold, flu, etc.), and especially if you think you might have COVID-19. It is important to take social responsibility and self-isolate until you test negative, after your symptoms have passed. Most people who contract COVID-19 will not need to be hospitalized, and as mentioned, can recover at home, as with any other upper respirator infection (cold or flu). However, you will need to self-quarantine yourself for at least 2 weeks, and possibly up to 4 weeks, until you test negative.
Above all, do NOT expose other people to the virus if you are sick with any contagious illness (cold, flu, etc.), and especially if you think you might have COVID-19. It is important to take social responsibility and self-isolate until you test negative, after your symptoms have passed. Most people who contract COVID-19 will not need to be hospitalized, and as mentioned, can recover at home, as with any other upper respirator infection (cold or flu). However, you will need to self-quarantine yourself for at least 2 weeks, and possibly up to 4 weeks, until you test negative.
Remember, only 15% of people infected with COVID-19 will develop complications, and with good medical care most will recover. Most of that 15% who develop complications will have underlying health conditions (asthma, emphysema, COPD, chronic bronchitis, heart failure, uncontrolled diabetes, etc.), be immuno-compromised, or be over the age of 80. If you are in these at-risk groups, do not hesitate to contact your doctor when you develop symptoms of COVID-19, particularly a spiking fever, coughing, and shortness of breath. You will need to be tested, and observed for complications. Due to limited space at the hospital, only those who develop complications will be admitted.
If you have not already started a quality nutritional supplement program, then consider it now, particularly if you are in a high-risk group. (See below for my suggestions.)
What Can We Expect Over the Next Six Weeks?
Based upon how the epidemic first spread in China, as well as how quickly it hopped to other countries, notably South Korea, Iran, and Italy, and is now spreading rapidly around the world, we have good idea of what to expect for what we will soon see in the U.S. [edit: what we are now seeing]. This virus will rapidly spread to every state and city, and soon be in nearly every community in the United States. The same goes for other countries. How fast it spreads, and the number of people who fall ill or die, will determine on the preventative actions taken.
Aggressive actions are now being taken in the United States, which will significantly mitigate the spread of the virus and drastically lower the number of deaths. As strange as this is for all of us, it is important not to panic, as this will not be a health disaster for most of us. However, it can be a nightmare due to people’s unwise, fearful, or greedy reactions.
There is NO REASON to hoard food and toilet paper. There is plenty to go around if people can just stop hoarding food and supplies. Since most people will not get sick, we could operate almost as we do normally in buying the supplies we need if fear did not overtake people. This is not the type of disaster that disrupts trucking and transportation as with a hurricane or winter storm.
Hospitals Will Be Overwhelmed Very Soon
 The problem with COVID-19 is the number of people who require hospitalization, particularly respiratory care in the Intensive Care Unit (ICU). Fortunately, in the United States, and most other first-world countries, have access to high-quality health care. Those who become very ill can get the care they need, as long as the hospitals do not become overwhelmed, as has already happened in Italy. Tents and open rooms with nothing more than cots and concrete floors are make-shift hospital rooms due to a lack of critical care beds. Many reports from Italy are that young people, even as young as 23, and without underlying medical illnesses, are requiring respiratory care. It is now time to take precautions seriously, and boost your immunity.
The problem with COVID-19 is the number of people who require hospitalization, particularly respiratory care in the Intensive Care Unit (ICU). Fortunately, in the United States, and most other first-world countries, have access to high-quality health care. Those who become very ill can get the care they need, as long as the hospitals do not become overwhelmed, as has already happened in Italy. Tents and open rooms with nothing more than cots and concrete floors are make-shift hospital rooms due to a lack of critical care beds. Many reports from Italy are that young people, even as young as 23, and without underlying medical illnesses, are requiring respiratory care. It is now time to take precautions seriously, and boost your immunity.
In Italy, there are so many people sick with COVID-19, they are overwhelming the hospitals, and the doctors’ and nurses’ ability to care for them. Doctors and nurses are getting sick with exhaustion and COVID-19.  They are having to make decisions about who will be put in the ICU or not, as there are too many severely sick people for the number of beds. In other words, they are deciding who will live and who will die. That could easily happen in the United States, Canada, and elsewhere, if we all do not take drastic measures to stop the spread of this virus.
They are having to make decisions about who will be put in the ICU or not, as there are too many severely sick people for the number of beds. In other words, they are deciding who will live and who will die. That could easily happen in the United States, Canada, and elsewhere, if we all do not take drastic measures to stop the spread of this virus.
The United States has 34.7 critical care beds per 100,000 people, with most of them already full with people sick with other illnesses. Italy is easily overwhelmed because they only have 12.5 critical care beds per 100,000 people, as does Canada. The U.K. has even fewer critical care beds, approximately 6.6 beds per 100,000 people. Those in the U.K., Canadians, Australians, Kiwis, and everyone in all countries, would do very well to take aggressive precautions VERY seriously, and protect themselves from the spread of this virulent virus.
Given the Reproduction Number (R0 ) of 2 – 2.5, the long incubation period (up to 14 days), the highly infectious nature of COVID-19, the ability to contract this by breathing in relatively few aerosolized contaminated droplets, or self-inoculate by touching contaminated surfaces, the fact that most people will only experience mild cold symptoms, combined with the reality that most people still will not wash their hands properly (if at all), and people will still shake hands, and that so many people will still go out when sick, and not take social responsibility seriously, this virus is bound to spread to your area by mid-April, if not the end of March. We all are about to know someone, even in our own families, who will test positive for COVID-19. We need to be prepared for it.
We may soon see imposed quarantines, as opposed to voluntary quarantines. There will be restrictions on gatherings in many cities. [Edit: this has happened since the time I started writing this article one week ago.] Schools will be closed, [ditto] and there will be a need for you to have at least a few weeks of food in your home for when human nature kicks in, and the panic buying starts to deplete the stocks on store shelves. [Edit: this happened faster than I thought.]
Prepare for a Possible Three-Week Quarantine, but You Do NOT Need a 3-Month Supply of Toilet Paper
 This is not written to cause panic, but so you can prepare for how fast this will unfold. And, please do not panic buy, and stock up on supplies beyond your current needs. Purchasing two months’ worth of toilet paper is just insanity, and clearing out the shelves of necessities while others go without, just to be able to sell them online for a profit is downright unethical; and if not criminal, it should be.
This is not written to cause panic, but so you can prepare for how fast this will unfold. And, please do not panic buy, and stock up on supplies beyond your current needs. Purchasing two months’ worth of toilet paper is just insanity, and clearing out the shelves of necessities while others go without, just to be able to sell them online for a profit is downright unethical; and if not criminal, it should be.
During this pandemic, as we go out and buy food and supplies, let’s remember who is most at risk. And, if we have an elderly neighbor, let’s offer to pick up supplies for them. We can look out for our neighbors, particularly those at risk.
If we take measures now to protect ourselves, including boosting our immune systems, and protect ourselves and others from fear, then we all can be in good shape. Let’s be prepared, and do so without the panic that can so easily befall us. Let’s all be better at exercising some not-so-common sense and long-forgotten courtesy.
Regarding health concerns, we absolutely do not need to panic, because, as I said several times, at least 85% of those who contract the virus will have only mild cold or flu-like symptoms, and most children will either not get it, or have a very mild sniffle or cough. It will appear nothing more than what happens normally to children.
This viral pandemic will get worse due to two reasons, the spread of the virus, and the more people getting tested, and the numbers will skyrocket (because more are being tested). Do not panic when you see this. By the end of April, if we take the proper precautions, and do our part, the spread of the virus should hit its peak, and level off. I predict by May, the numbers of new cases will begin to decline, and dramatically fall off by June. We may see the tail end of this pandemic in the United States by July. I hope it is earlier, and pray that it does not drag out longer, and with as few lives lost as possible. However, not all will see the end. But, we can make a difference, if we take precautions now.
What are the Best Precautions to Reduce Risk of Acquiring and Spreading COVID-19?
If you watch the media right now, you will see precaution recommendations issued from the WHO and the CDC. I agree with almost all of them, which you can find at coronavirus.com. However, I slightly differ on a few points, which you will read below. And most importantly, I have suggestions for nutritional supplements to consider for supporting your immune system, which I truly believe can help, based upon my 25 years of experience with using and recommending quality supplements, beginning in my medical practice.
Precautions Against Self-Inoculation
 Since at least half of the cases of COVID-19 are transmitted through self-inoculation after touching a contaminated surface and then your face, the answer is of course, WASH YOUR HANDS WITH SOAP before touching your face.
Since at least half of the cases of COVID-19 are transmitted through self-inoculation after touching a contaminated surface and then your face, the answer is of course, WASH YOUR HANDS WITH SOAP before touching your face.
If you teach your family, especially your children who go to school, and touch kids, desks, tables, doorknobs, etc., who themselves have been touched by many others, who come from several hundred families, then you can imagine how schools are the perfect place to spread a communicable disease. This is why schools will need to be closed to help end the pandemic. [Edit: This is happening now.]
Have you ever thought about what your children bring back on their hands every day from school, when they enter your home? Often the first thing they go for is the refrigerator handle, along with others, and is it any wonder the whole household gets sick within days?
This should not ever have needed to have been said, but apparently 35% of the population never got the memo, but PLEASE wash your hands with soap and water (for 20 to 30 seconds) after using the bathroom, ESPECIALLY after a bowel movement. Nobody wants to be handling your feces, nor having you spread your fecal material around on various surfaces you touch. If you wash off your fecal bacteria, you will also help wash off COVID-19 and the influenza virus.
Wash Your Hands with Soap for 20 to 30 Seconds
- After using the restroom
- Before touching your face
- After touching a public surface
- After handling money
- Every time you enter your home
- After touching someone
- After touching someone’s property
No matter how much it can be emphasized, unfortunately, there are still going to be people who will not wash their hands, even after getting sick with the coronavirus.
In addition to washing your hands with soap and water for 20 to 30 seconds, it is important to sani-wipe down all commonly touched surfaces in your home, car, and other places that seem appropriate. If you want to protect your family from the coronavirus, influenza, and other cold viruses, sani-wipe commonly touched surfaces daily, if not twice daily for commonly touched surfaces in busy households with young children.
Sani-Wipe These Commonly Touched Surfaces Daily (if Not Twice Daily)
- Doorknobs
- Faucet handles
- Flush levers
- Light switches
- Refrigerator handles
- Tables
- Chair backs
- Counter tops
- Handrails
- TV Remotes (be careful to not let liquids enter electronics)
- Keypads (be careful to not let liquids enter electronics)
- Cell phones (caution: alcohol-based wipes will wear off the smooth, smudge-free oleophobic surface on glass)
- Car: door handles, arm rests, car seats, steering wheel, seatbelt buckle, especially after kids in car
- ATM/Grocery Store Keypads (take small package of sani-wipes with you, everyone will appreciate it)
- Grocery carts
- Airplane seat and armrest, tray, and in-seat touchscreen
Precautions Against Aerosolized Transmission
 Obviously, even without a pandemic, everyone should be covering their coughs and sneezes (into throw-away tissues or one’s elbow). Do not cough or sneeze into your hand, as you will just touch objects, and spread bacteria and viruses virtually anywhere. Exercise common sense, and take responsibility for yourself and others.
Obviously, even without a pandemic, everyone should be covering their coughs and sneezes (into throw-away tissues or one’s elbow). Do not cough or sneeze into your hand, as you will just touch objects, and spread bacteria and viruses virtually anywhere. Exercise common sense, and take responsibility for yourself and others.
Since COVID-19 remains active in micro droplets of saliva that can remain suspended in the air for at least 3 hours, and possibly up to 9 hours, the chance of you inhaling contaminated saliva micro droplets in a crowd of people in most cities in the United States by the end of March is quite high.
Even if this highly infectious virus was viable in aerosolized micro droplets for only 10 minutes, that is plenty of time for you to unknowingly walk into the micro spray of a sneeze from a person you never saw. Remember, it does not take many viruses with COVID-19 to cause infections, which is why you need to avoid confined, crowded spaces, which are the greatest risk for inhaling contaminated micro saliva droplets. If they cannot be avoided, then wear a N95 or N99 mask.
It is time to practice social distancing. This is actively happening in Italy, which was hit hard. When standing in lines, they are standing at least 6 feet away from each other. We are not used to this, and it cannot always be avoided, but as best you can, it is time to be more aware of distancing yourself from crowds over the next 4 to 6 weeks.
You may wish to spend more time at home, and if possible, work from home. And above all, avoid unwittingly infecting those who are high risk.
What About Wearing a Mask?
 The recommendations from the CDC, and what you have seen reported on TV, is “not to wear a mask.” Well, the reason for that is not because proper masks do not protect you from inhaling the virus, but because there is a shortage of masks coming in from China, and they are needed for healthcare workers.
The recommendations from the CDC, and what you have seen reported on TV, is “not to wear a mask.” Well, the reason for that is not because proper masks do not protect you from inhaling the virus, but because there is a shortage of masks coming in from China, and they are needed for healthcare workers.
Most medical supplies, like gloves and masks, now come from China, and they were needed in China, and with the high demand, a shortage has been created. This is the reason for the recommendations for the public not to wear a mask. Believe me, if there were plenty of masks to go around, the recommendations would be to wear a mask when you are in crowds, or even when you go out in public, just as they are now worn in hospitals.
A surgical mask helps reduce the distance that saliva droplets are expelled from you speaking, coughing, and sneezing; and helps reduce the frequency of you touching your mouth and nose. However, surgical masks do not provide good protection against inhaling the virus, which can enter through the sides of the masks, as the masks do not fit tightly on all areas of the face. In addition, the material of the surgical mask is not designed to filter viruses.
N95 and N99 masks are designed to filter very small particles the size of viruses, which is why they can stop the coronavirus (and all other viruses). N95 masks are often used by those working with fine dust particles.
There are N95 masks that come with exhale valves (such as the 3M mask), which reduces heat and moisture from building up inside the mask.
Regarding Wearing a Mask
 Fact 1: COVID-19 will be in all major cities, and then some, by the end of March, and definitely by mid April, if it is not in your area already.
Fact 1: COVID-19 will be in all major cities, and then some, by the end of March, and definitely by mid April, if it is not in your area already.
Fact 2: COVID-19 is highly infectious (approximately 20 times more than SARS), and is transmitted via aerosolized micro droplets.
Fact 3: You can contract COVID-19 via aerosolization from others even if you are not in their immediate proximity, as it can remain viable in the air for 30 minutes to 3 hours.
Fact 4: You are most likely to contract COVID-19 in crowded and confined areas.
Fact 5: Those over the age of 60, the immuno-compromised, and those with underlying chronic illnesses are at increased risk of severe complications and death due inhaling the COVID-19 virus.
Fact 6: N95 and N99 masks protect you from inhaling the COVID-19 virus (as well as other viruses), if you wear them while out in public, especially while near others.
Draw your own conclusions as to whether you should wear a mask or not, but I think it is prudent to do so while out in public, especially if you are in an at-risk group.
What Other Precautions Should You Consider?
 When COVID-19 hits your area in the next 2 weeks (if it has not already), and if you are immuno-compromised, have an underlying lung disease, such as asthma, chronic bronchitis, COPD, emphysema, or other chronic diseases, such as heart disease, or uncontrolled diabetes, or over the age of 80, prepare now to self-isolate. In other words, stay at home, and if you go out, avoid crowds and wear the appropriate mask. Beware of all those entering your home, as people can be contagious without even knowing it. Consider severely restricting visitors for the next 6 weeks. And if you do, consider having them wear an N95 mask, wash their hands, and not touch you.
When COVID-19 hits your area in the next 2 weeks (if it has not already), and if you are immuno-compromised, have an underlying lung disease, such as asthma, chronic bronchitis, COPD, emphysema, or other chronic diseases, such as heart disease, or uncontrolled diabetes, or over the age of 80, prepare now to self-isolate. In other words, stay at home, and if you go out, avoid crowds and wear the appropriate mask. Beware of all those entering your home, as people can be contagious without even knowing it. Consider severely restricting visitors for the next 6 weeks. And if you do, consider having them wear an N95 mask, wash their hands, and not touch you.
Pregnant Women Take Precautions
Pregnant women should consider self-isolation when the coronavirus comes to your area, and should wear an N95 or N99 mask when going out in public or to the doctor’s office. Fortunately, from all reports of pregnant women who delivered babies while actively sick with COVID-19, none of the babies were negatively affected.
At-Risk Population Start Self-Isolation and Aggressive Precautions Now
If you have any of these underlying health conditions (above), and work in an industry in which you are exposed to a lot of people, consider a 3-month sabbatical now, and prepare for self-isolation at home, with all the precautions mentioned.
The gym is a particularly risky place for transmitting bacteria and viruses, due to the wet, warm air and surfaces. In addition, people are breathing heavily, and putting out more saliva micro droplets. (The virus does not come out in your sweat, but can remain alive in micro droplets of saliva mixed with micro droplets of sweat.) Consider exercising at home or outdoors away from crowds until the pandemic has passed.
When COVID-19 comes to your area, and it will, decide if you are going to have visitors enter your home, and what you will ask of them. Will you ask them to wash their hands, or use hand sanitizer? Will you ask them if they have been sick or had recent contact with others who have been sick? Your home is the one thing that you have the most control over, so decide how seriously you are going to take this pandemic.
What About Killing the Coronavirus with a Blow Dryer?
There is a video going around about using a blow dryer (or getting in a sauna) to kill the coronavirus. This is a limited situation, and if it helps, it would only help while only having viral sinusitis, not once it got into the lungs and caused a cough.
It is true that coronaviruses (and other viruses) are killed at 133 F and above, and that exposing the virus to those temperatures for 2 minutes would kill viruses. However, breathing in hot air from a blow dryer through your nose to kill a lung infection does not make sense. By the time a person has a fever and a cough, COVID-19 (or any respiratory virus), has already infected the epithelial cells of the aveolar cells in the lungs. The air that makes it down into your lungs cannot remain hot enough, nor for a long enough time to kill the viruses and you being able to tolerate it. Yes, it could theoretically kill viruses in your nasal passages (as described in the video) if the infection was only in your nose, but once in the lungs, this virus attaches to ACE2 receptors in the aveoli, and that is the real concern of this this respiratory virus. If caught early, it might work.
What About Travel?
 Now is not the time to take a cruise. Other travel should be restricted to only that which is necessary, if we are going to stop this growing pandemic. Soon we may not have a choice when the virus hits its peak at the end of March-to-Mid-April.
Now is not the time to take a cruise. Other travel should be restricted to only that which is necessary, if we are going to stop this growing pandemic. Soon we may not have a choice when the virus hits its peak at the end of March-to-Mid-April.
Subways, trains, buses, cruise ships, are all crowded, confined spaces, and are high-risk areas to contract COVID-19. If you want to avoid contracting this virus, then you will need to avoid these methods of transportation. If you do not have much choice, then consider all the aggressive precautions above.
Even if you are relatively young and healthy, and despite only having the risk of having mild cold or flu-like symptoms, if you catch the virus, you may end up quarantined for 2 weeks or more. Worse than you being quarantined, is that if you catch COVID-19, and then transmit it to someone who dies because you did not take it seriously, or simply do not care, and did not want to be inconvenienced by washing your hands, self-isolating when sick, or any other of these recommended precautions, what does that say about you? Please don’t be that person.
Airplanes are equipped with quality ventilation systems, including HEPA filters that trap viruses. The ventilation system is sectional, and the air flow is from the ceiling to the floor, which helps reduce turbulence, and moving particulate matter away from your face. All this is good, but… what is to stop someone sitting near you coughing or sneezing on you, or the surfaces from being contaminated during the flight? [Edit: Of course, hardly anyone is flying right now, so it could be that airplanes are relatively safe at the moment.]
If you have to fly, sani-wipe everything in your area as you get to your seat, and even during your flight, as needed.
If you have an underlying health conditions, especially over the age of 60, do not fly if unnecessary.
What Nutritional Supplements Support the Immune System?
 I want to make this clear. I am not claiming that any supplement can prevent or treat a COVID-19 infection. There is no research to support this yet. However, given how studies have shown that several micronutrients exert anti-viral activity against viruses that cause the common cold (upper respiratory tract infections), namely rhinoviruses and coronaviruses, and with some micronutrient derivatives having been found to exhibit antiviral activity against the SARS coronavirus, we can assume that various micronutrients are very likely going to have a similar encouraging impact against COVID-19 (SARS-CoV-2) infections.
I want to make this clear. I am not claiming that any supplement can prevent or treat a COVID-19 infection. There is no research to support this yet. However, given how studies have shown that several micronutrients exert anti-viral activity against viruses that cause the common cold (upper respiratory tract infections), namely rhinoviruses and coronaviruses, and with some micronutrient derivatives having been found to exhibit antiviral activity against the SARS coronavirus, we can assume that various micronutrients are very likely going to have a similar encouraging impact against COVID-19 (SARS-CoV-2) infections.
There are many micronutrients (vitamins, minerals, antioxidants, etc.) that research has shown are very beneficial to our health, and in particular, very beneficial to our immune systems.
Research Shows Reduction in Viral Upper Respiratory Infections with Various Vitamins and Antioxidants
Research has shown that various micronutrients are associated with a reduction in the incidence of colds and influenza, particularly vitamin D. (11 – 16) The lower one’s vitamin D level, the higher the prevalence of upper respiratory tract infections from the viruses that cause colds (coronaviruses and rhinoviruses), and influenza. And a single high-dose of vitamin D, combined with antibiotics has been shown to improve, that is accelerate the complete resolution of pneumonia. (17)
Animal models are useful for studying the results of micronutrients, as it allows researchers to cause illness, and observe the direct results of treatment. Such studies have shown that various antioxidants, such as alpha lipoic acid, vitamin C, and vitamin E are beneficial in the premedication of Acute Respiratory Distress. In other words, if antioxidants are already in the system, treatment of Acute Respiratory Distress is more effective. (18)
Of course, we need to do more than just take nutritional supplements, such as eat well, get regular restorative sleep, reduce stress, exercise, maintain a healthy weight, not smoke, use alcohol in moderation or not at all, etc. All these factors affect your immune system’s ability to keep you healthy.
Viral upper respiratory tract infections occur frequently in young people who are overly stressed. The immune system is suppressed from excessive exercise, emotional stress, and lack of sleep. One case study showed that a combination of improved sleep, vitamin D supplementation, along with quercetin (a flavonoid antioxidant) significantly reduced the frequency of recurrent upper respiratory tract infections. (19)
Various Flavonoid Antioxidants, Such as Quercetin, Stilbenes, and Grape Seed Extract, Demonstrate Anti-Viral Activity
 Flavonoid antioxidants, such as quercetin and resveratrol exhibit anti-viral activity against common viruses that cause upper respiratory tract infections, including influenza A (H1N1) and B. (20 – 26) Of note, stilbene derivatives, (including resveratrol), quercitin derivatives, and the compounds found in green tea extract, have shown anti-viral activity against the SARS coronavirus. (27 – 30) Since COVID-19 is essentially SARS2, you cannot blame anyone using such micronutrients at this time.
Flavonoid antioxidants, such as quercetin and resveratrol exhibit anti-viral activity against common viruses that cause upper respiratory tract infections, including influenza A (H1N1) and B. (20 – 26) Of note, stilbene derivatives, (including resveratrol), quercitin derivatives, and the compounds found in green tea extract, have shown anti-viral activity against the SARS coronavirus. (27 – 30) Since COVID-19 is essentially SARS2, you cannot blame anyone using such micronutrients at this time.
Grape seed extract (proanthocyanidin bioflavonoid) exhibit potent antioxidant capacity, as well as anti‑bacterial, anti‑viral, anti‑carcinogenic, anti‑inflammatory and anti‑allergic actions. One significant way respiratory viruses cause death is by causing an overwhelming system-wide inflammation, known as cytokine storm. Respiratory viruses cause inflammation in the epithelial cells of the lungs (as does COVID-19), and increase the risk of respiratory distress and pneumonia. Grape seed extract inhibits the abnormal release of proinflammatory cytokines caused by the virus. (31)
I have been recommending high quality supplements to my patients since 1995, and although retired from medical practice, I have been actively researching nutritional supplements for over 25 years. If you knew what I know about the benefits of quality supplements, you would never miss a day of taking what I take, especially now with this pandemic; particularly if you have an underlying chronic illness.
We know that a low immunity increases the risk of infections, and it stands to reason, that boosting immunity will give you a fighting chance to remain healthy. If nothing else, if you get sick, by boosting immunity, your immune system will be primed to deal with viruses and bacteria, and have the energy needed to cope with the illness, reduce the risk of complications, and shorten the recovery time.
Although, I have been taking a wide range of quality nutritional supplements, twice daily for over 25 years, since COVID-19 first started showing in the U.S, I increased the dose of certain supplements that I have already been taking, particularly a quality beta glucan supplement with zinc, and a quality grape seed extract with vitamin C. If you are not yet taking quality nutritional supplements, such as what I listed below, consider doing so, after first consulting with your own licensed health care professional, of course.
Beta Glucan Supplement

Biologically-active beta glucan polysaccharides are one of the most studied micronutrient immunomodulators that have multiple modes of action. According to many studies, they exert immunomodulatory, anti-inflammatory, anti-carcinogenic, anti-fungal, anti-bacterial, and anti-viral activity, and are therefore an obvious choice for preventing and treating upper respiratory tract infections caused by the rhinoviruses and coronaviruses. (32) Beta glucans have proven therapeutic and preventive anti-viral effects against respiratory tract infections in children, adults, and elite athletes. (33)
Beta glucans are fiber polysaccharides derived from the cell membranes of the reishi and shiitake mushrooms, as well as from baker’s yeast extract (Saccharomyces cerevisiae). These polysaccharides (chains of sugar molecules) do not breakdown in the stomach, and therefore do not have any impact on blood glucose levels, nor provide calories. The molecules pass into the intestines and then bloodstream, where they exert their effects on the white blood cells of the immune system.
Beta Glucans Activate Various White Blood Cells
Beta glucan polysaccharides directly modulate (activate or trigger) white blood cells, called macrophages, to more effectively attack and kill bacteria, mold/yeast, viruses, and cancer cells. In addition, through cytokine cell signaling, beta glucans trigger B lymphocytes and Cytotoxic T Lymphocytes (another type of white blood cells), to activate a complement and antibody response, to create a “one-two” knock-out punch to kill bacteria, cancer cells, viruses, and cells infected with viruses. Through triggering cell-signaling messenger cytokines, beta glucans trigger other white blood cells, called Natural Killer Cells to be armed with cytotoxic chemicals to be able to destroy bacteria, mold/yeast, viruses, and cancer cells.
Beta glucans have been shown to reduce the number of viral upper respiratory tract infections (common colds, which are caused by rhinoviruses and coronaviruses), and even improves mood. (34) One study among people between the ages of 50 – 70, showed that daily supplementation with beta glucans protected against contracting viral upper respiratory tract infections, and reduced the duration of the symptoms once infected. (35)
Beta Glucans Modulate a Healthy Immune Response and Prevent Cytokine Storm
Beta glucans heighten, or sharpen the immune response when needed, without causing an over-reaction.
Viral and bacterial respiratory infections can cause organ failure and death through causing widespread inflammation, known as cytokine storm. Cytokines are cell signaling biochemicals, some of which are pro-inflammatory. Cytokines recruit white blood cells to fight infections. Beta glucans cause a normal physiological release of pro-inflammatory cytokines for the recruitment of white blood cells. Most significantly, beta glucans also help prevent the over-reaction caused by the virus, specifically, cytokine storm. (36)
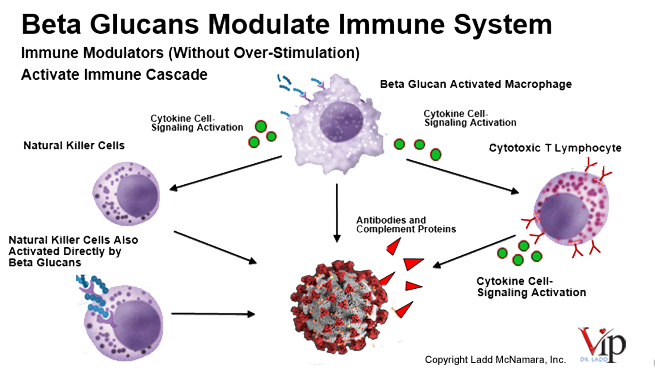
In addition to their anti-microbial, anti-viral, and anti-fungal effect, beta glucan polysaccharides demonstrate anti-obesity, anti-diabetic, and anti-cancer properties. The first mechanisms of action begins in the gut, where the beta glucans act as prebiotics for the digestive bacteria (probiotics). In addition beta glucans exert antioxidant, anti-inflammatory, and additional immuno-modulating activities.
Micronutrients Work Synergistically with Other Micronutrients
Beta glucans work synergistically with other supplements, to work better together to prevent and fight infections of all types. Various micronutrients work synergistically with beta-glucan, such as vitamin D, vitamin C, resveratrol, quercetin, elderberry extract, and grape seed extract.
From all that I have studied and experienced, beta glucans are so powerful in exerting antiviral activity, I believe this is one critical supplement to be taking at this time.
Organ transplant recepients should NOT take beta glucans, on the chance that beta glucans may cause the immune system to overcome the immuno-suppressant medications and damage the transplanted organ.
For those with an autoimmune disease, you may wish to avoid beta glucan supplements on the theoretical risk of causing the immune system to flareup. However, from all reports I have heard for over three years now, those with autoimmune disorders who are taking 550 mg of beta glucan polysaccharides per day are not experiencing flareups. I only make this warning out of an abundance of caution.
It is imperative to understand that I am providing my suggestions and considerations as information only, not as medical advice. Please see the medical disclaimer in the footer about consulting with your personal physician.
Probiotics
 Probiotics are beneficial bacteria that inhabit our intestines. They are among many bacteria that make up our microbiome. Among many roles that the microbiome plays, supporting the immune system is a critical one. (37, 38)
Probiotics are beneficial bacteria that inhabit our intestines. They are among many bacteria that make up our microbiome. Among many roles that the microbiome plays, supporting the immune system is a critical one. (37, 38)
Most people do not have a healthy, or at least optimal microbiome. To support your gastro-intestinal tract, reduce gas, bloating, diarrhea, constipation, improve digestion, improve mood, and support your immune system, consider taking probiotics daily.
The probiotics that have scientifically shown to be beneficial to seed the microbiome, to create a beneficial milieu for other beneficial bacteria to flourish, and stave off the bad bacteria, provide numerous benefits, including reducing upper respiratory infections, are Bifidobacterium BB-12 and Lactobacillus rhamnosus LGG. (39 – 42) These two strains can remain viable for up to 18 months at room temperature, and they survive the harsh acidic environment of the stomach, and pass into the intestines to duplicate rapidly to establish a healthy microbiome.
A Boost of Vitamin C with Elderberry Extract, Zinc, and Echinacea
Another supplement that may provide beneficial effects for respiratory infections, at least in the short-term (8 weeks or less), is echinacea. Studies are mixed on its benefits, but it is seems to be more effective when combined with other micronutrients, particularly when combined with vitamin C, zinc, and elderberry extract. (43 – 46)
Since echinacea should not be used for more than 8 weeks, as it may elevate liver enzymes, or have a negative effect on immunity, I suggest reserving this supplement when actually feeling an illness coming on.
Dr. Ladd’s Nutritional Supplement Considerations to Support Your Immune System
The following is the basic protocol for supporting the immune system. This is not intended as medical advice, but as information only. Please consult your own personal physician prior to starting a supplement regimen. Please read full disclaimer in the footer of this webpage.
Note: When taking supplements, remember that quality pure raw ingredients and quality manufacturing of potent supplements make a huge difference in effectiveness. Not all supplements are created equally.
 Wide-Spectrum of Vitamin-Antioxidant Supplement, (preferrably one that also includes quercetin, resveratrol, curcumin, olive extract, among many other micronutrients), Twice Daily
Wide-Spectrum of Vitamin-Antioxidant Supplement, (preferrably one that also includes quercetin, resveratrol, curcumin, olive extract, among many other micronutrients), Twice Daily- Multi-Mineral Supplement, (one that provides selenium, zinc, calcium, magnesium, mangenese, as well as many other minerals), Twice Daily
- Pure Fish Oil, Twice Daily
- Vitamin D, 6000 – 10,000 IU (150 – 250 mcg) per day
- Grape Seed Extract, 200 – 400 mg, Twice Daily
- Beta Glucan Polysaccharide (extracts derived from reishi and shiitake mushrooms, as well as baker’s yeast extract, preferably with zinc) 225 – 550 mg, Twice Daily.
- Probiotics, (Bifidobacterium BB-12 and Lactobacillus rhamnosus LGG), Once per Day.
If you are not sure what quality brand to take, feel free to contact me regarding what I take, knowing that there is no claim being made that it can prevent or cure COVID-19.
Conclusion
Do not fear, do not panic, and do not hoard. Let’s be aware of those most at risk, and be kind to one another. Most of all, let’s not allow ourselves to knowingly put others at risk. We can mitigate this pandemic, by protecting ourselves and others. We are all in this together, and together we will get through this.
Everything on this website is for informational purposes only, and not intended as medical advice. Consult your physician before starting nutritional supplements. Please read the full medical disclaimer via the link in the footer below.
References
- Lu R, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020 Feb 22;395(10224):565-574.
- Zhou P, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020 Feb. [E-publication ahead of print]
- “Don’t Buy China’s Story: The coronavirus may have leaked from a lab.” New York Post article, Feb 22, 2020, by Steven Mosher. https://nypost.com/2020/02/22/dont-buy-chinas-story-the-coronavirus-may-have-leaked-from-a-lab/
- “Virus-hit Wuhan has two laboratories linked to Chinese bio-warfare program.” Washington Times, Jan 24, 2020, by Bill Gertz. https://www.washingtontimes.com/news/2020/jan/24/virus-hit-wuhan-has-two-laboratories-linked-chines/
- Bourouiba L, et al. Violent expiratory events: on coughing and sneezing. J, Fluid Mechanics. 2014 Apr;745:537-563.
- “Coronavirus can travel twice as far as official ‘safe distance’ and stay in air for 30 minutes, Chinese study finds.” South China Morning Post, Mar 9, 2020, by Stephen Chen. https://www.scmp.com/news/china/science/article/3074351/coronavirus-can-travel-twice-far-official-safe-distance-and-stay
- Kampf G, et al. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020 Mar;104(3):246-251.
- NIH Report, March 3, 2020 https://www.nih.gov/news-events/nih-research-matters/novel-coronavirus-structure-reveals-targets-vaccines-treatments
- CDC Coronavirus Information Precautions, etc. found at coronavirus.gov
- Welch D, et al. Far-UVC light: A new tool to control the spread of airborne-mediated microbial diseases. Sci Rep. 2018 Feb 9;8(1):2752.
- Arihiro S, et al. Randomized Trial of Vitamin D Supplementation to Prevent Seasonal Influenza and Upper Respiratory Infection in Patients With Inflammatory Bowel Disease. Inflamm Bowel Dis. 2019 May 4;25(6):1088-1095.
- Loeb M, et al. Effect of Vitamin D supplementation to reduce respiratory infections in children and adolescents in Vietnam: A randomized controlled trial. Influenza Other Respir Viruses. 2019 Mar;13(2):176-183.
- Pham H, et al. Acute Respiratory Tract Infection and 25-Hydroxyvitamin D Concentration: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2019 Aug 21;16(17).
- Zhou YF, et al. The association between vitamin D deficiency and community-acquired pneumonia: A meta-analysis of observational studies. Medicine (Baltimore). 2019 Sep;98(38):e17252.
- Ginde AA, et al. Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch Intern Med. 2009 Feb 23;169(4):384-90.
- Cannell JJ, et al. Epidemic influenza and vitamin D. Epidemiol Infect. 2006 Dec;134(6):1129-40.
- Slow S, et al. Effect of adjunctive single high-dose vitamin D3 on outcome of community-acquired pneumonia in hospitalised adults: The VIDCAPS randomised controlled trial. Sci Rep. 2018 Sep 14;8(1):13829.
- Erol N, et al. The Protection Potential of Antioxidant Vitamins Against Acute Respiratory Distress Syndrome: a Rat Trial. Inflammation. 2019 Oct;42(5):1585-1594.
- Ranchordas MK, et al. Case Study: Nutritional and Lifestyle Support to Reduce Infection Incidence in an International-Standard Premier League Soccer Player. Int J Sport Nutr Exerc Metab. 2016 Apr;26(2):185-91.
- Nile SH, et al. Probing the effect of quercetin 3-glucoside from Dianthus superbus L against influenza virus infection- In vitro and in silico biochemical and toxicological screening. Food Chem Toxicol. 2020 Jan;135:110985.
- Somerville VS, et al. Effect of Flavonoids on Upper Respiratory Tract Infections and Immune Function: A Systematic Review and Meta-Analysis. Adv Nutr. 2016 May 16;7(3):488-97.
- Vaidya B, et al. Effectiveness of Periodic Treatment of Quercetin against Influenza A Virus H1N1 through Modulation of Protein Expression. J Agric Food Chem. 2016 Jun 1;64(21):4416-25.
- Li C, et al. In vitro antiviral effects and 3D QSAR study of resveratrol derivatives as potent inhibitors of influenza H1N1 neuraminidase. Chem Biol Drug Des. 2015 Apr;85(4):427-38.
- Drago L, et al. In vitro antiviral activity of resveratrol against respiratory viruses. J Chemother. 2008 Jun;20(3):393-4.
- Friel H, Lederman HA. nutritional supplement formula for influenza A (H5N1) infection in humans. Med Hypotheses. 2006;67(3):578-87.
- Varricchio AM, et al. Resveratrol plus carboxymethyl-β-glucan in children with recurrent respiratory infections: a preliminary and real-life experience. Ital J Pediatr. 2014 Nov 23;40:93.
- Li YQ, et al. Synthesis of stilbene derivatives with inhibition of SARS coronavirus replication. Eur J Med Chem. 2006 Sep;41(9):1084-9.
- Nguyen TT, et al. Flavonoid-mediated inhibition of SARS coronavirus 3C-like protease expressed in Pichia pastoris. Biotechnol Lett. 2012 May;34(5):831-8.
- Park HR, et al. Synthesis and antiviral evaluation of 7-O-arylmethylquercetin derivatives against SARS-associated coronavirus (SCV) and hepatitis C virus (HCV). Arch Pharm Res. 2012 Jan;35(1):77-85.
- Chen L, et al. Binding interaction of quercetin-3-beta-galactoside and its synthetic derivatives with SARS-CoV 3CL(pro): structure-activity relationship studies reveal salient pharmacophore features. Bioorg Med Chem. 2006 Dec 15;14(24):8295-306.
- Kim SJ, et al. Pretreatment with a grape seed proanthocyanidin extract downregulates proinflammatory cytokine expression in airway epithelial cells infected with respiratory syncytial virus. Mol Med Rep. 2019 Apr;19(4):3330-3336.
- Friedman M. Mushroom Polysaccharides: Chemistry and Antiobesity, Antidiabetes, Anticancer, and Antibiotic Properties in Cells, Rodents, and Humans. Foods. 2016 Nov 29;5(4).
- Jesenak M, et al. Respiratory Tract Infections and the Role of Biologically Active Polysaccharides in Their Management and Prevention. Nutrients. 2017 Jul 20;9(7).
- Talbott SM, Talbott JA. Baker’s yeast beta-glucan supplement reduces upper respiratory symptoms and improves mood state in stressed women. J Am Coll Nutr. 2012 Aug;31(4):295-300.
- Fuller R, et al. Yeast-derived β-1,3/1,6 glucan, upper respiratory tract infection and innate immunity in older adults. Nutrition. 2017 Jul – Aug;39-40:30-35.
- Bedirli A, et al. Beta-glucan attenuates inflammatory cytokine release and prevents acute lung injury in an experimental model of sepsis. Shock. 2007 Apr;27(4):397-401.
- Ashraf R, Shah NP. Immune system stimulation by probiotic microorganisms. Crit Rev Food Sci Nutr. 2014;54(7):938-56.
- Kechagia, M, et al. 2013. Health benefits of probiotics: a review. ISRN Nutr [Internet] [accessed 4 June 2018] Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4045285/#B3
- Jungersen M, et al. The Science behind the Probiotic Strain Bifidobacterium animalis subsp. lactis BB-12®. Microorg 2014 2:92-110.
- Tancrède C. Role of human microflora in health and disease. Eur J Clin Microbiol Infect Dis 1992 11(11):1012-5.
- de Vrese M, et al. Effect of Lactobacillus gasseri PA 16/8, Bifidobacterium longum SP 07/3, B. bifidum MF 20/5 on common cold episodes: a double blind, randomized, controlled trial. 2005 Clin Nutr 24(4):481-91.
- Smith TJ, et al. Effect of Lactobacillus rhamnosus LGG® and Bifidobacterium animalis ssp. lactis BB-12® on health-related quality of life in college students affected by upper respiratory infections. Br J Nutr. 2012, Oct 1:1-9.
- Schapowal A, et al. Echinacea reduces the risk of recurrent respiratory tract infections and complications: a meta-analysis of randomized controlled trials. Adv Ther. 2015 Mar;32(3):187-200.
- Rerksuppaphol S, Rerksuppaphol L. A randomized controlled trial of zinc supplementation in the treatment of acute respiratory tract infection in Thai children. Pediatr Rep. 2019 May 23;11(2):7954.
- Tiralongo E, et al. Elderberry Supplementation Reduces Cold Duration and Symptoms in Air-Travellers: A Randomized, Double-Blind Placebo-Controlled Clinical Trial. Nutrients. 2016 Mar 24;8(4):182.
- Krawitz C, et al. Inhibitory activity of a standardized elderberry liquid extract against clinically-relevant human respiratory bacterial pathogens and influenza A and B viruses. BMC Complement Altern Med. 2011 Feb 25;11:16.
- Fang L, et al. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020 Mar 11.
- Day, M. COVID-19: ibuprofen should not be used for managing symptoms, say doctors and scientists BMJ 2020;368:m1086. (Click here for link.)


{kind=link}
Thank you for this great information Dr Ladd McNamara
Thank you so much Carole.
Thank you, Dr. Ladd, for a thorough understanding and explanation of what we need to know going forward.
Thanks for the information and peace of mind.
Be well!
Dyann and Wild
Thank you so much Dyann. I appreciate your kind comment.
Thank you for the timely posting of this information with regards to danger of COVID 19 & corresponding suggestion 0n what nutritional supplement to guard against this pandemic!
Thank you so much Winston
Thank you so much Dr. Ladd for this very nicely put together and thorough article 🙂🤗❤️🥰
Thank you so much Teresa
Great summary, Dr. Ladd!
Thank you Deb
Thank you Dr. Ladd McNamara for such a through explanation. I’ve shared this many times and including myself you’ve calmed many fears.
I appreciate your time and wanting to help others who have no idea what this all means understand it.
I don’t have a scientific mind so this is just an awesome!
You are very much appreciated, as this must have taken you a long time to do.
Finally, a reasonable perspective without the drama.
Thank you so much Judyann, I appreciate that feedback more than you know.
Excellent Ladd! Thank You.
Finally we have one place to get all of the facts.
Appreciate all you do!
Thank you so much Maggie.
Just read an article published by France that says we should avoid antiinflamatorio medicine and supplements
https://www.theguardian.com/world/2020/mar/14/anti-inflammatory-drugs-may-aggravate-coronavirus-infection?fbclid=IwAR2GycBvB7FzknNlnZEUOnO5sgb7Z3-NusoloYPF8YOh7PlWW755ueX7EJ4
Yes, I included this topic within my article; you will see that I suggest for people who have symptoms, to choose Tylenol instead of ibuprofen. It is anecdotal evidence, but we have a choice, so error on side of caution.
Very interesting from the UK.
There seems to be a lot of mass hysteria at the moment. After the announcement from our government yesterday everyone has lost their mind.
Some of the information you’ve mentioned would be very useful in the media.
Would you be able to provide a good daily routine of supplements alongside my diet please? I am quite healthy as it is so looking for additions.
Thank you
Michael, Feel free to email me, and I will let you know what I take.
Dr. Ladd, thank you for taking the time to do the research. This is the best article I’ve read so far in regards to the facts and a clear understanding of what to do to contribute to this pandemic we are all experiencing.
Thank you Susan.
Hi I am interested in the specific brand supplements you are taking. Could you share this information? Thank you for this article it really has given me some oeace of mind.
Melissa, Thank you so much. Feel free to email me, and I will let you know what I take.
I apologize. I thought I had answered you. Feel free to email me, and I will let you know what I take.
Thank you for donating so much of your time and expertise to help others. This is a very comprehensive article.
Thank you so much.
Although this reply is way late; thank you for your kind comment.
Well written, very knowledgeable, extremely informative, factual and timely information. I’ve shared with family, friends and staff. Hopefully we’ll flatten the curve sooner than later.
In good health!
I agree about hope for flattening the curve. Thank you so much for your kind compliments.
Wow, thank you so much for this very helpful article. Took a little time to read and digest (I printed and highlighted sections), but well worth the time. I appreciate the fact based information and helpful and hopeful recommendations.
Thank you so much. Glad it was helpful.
Forgive me for my delayed reply; I thought I had thanked you already. Thank you so much. Your kind comment is very much appreciated. Be well.
Thank you Dr Ladd for all the time and energy you have spent in researching information for all of us! God bless you! Rita
Thank you so much.
Rita, I thought I had thanked you previously. I don’t see it now; so thank you again for your kind comment.
Thank you so much for this information it is extremely useful and clears up many of my unanswered questions. I am currently breastfeeding and would like to know which vitamins and brands are safe to take while doing so. I am a nurse and would like to build a strong immune system for what is to come .
Amy, the protocol for immune support in pregnancy includes what is in the link. It is the brand I use. Feel free to email me, and I will let you know.
I apologize for my delayed response. I thought I had already replied to you. Feel free to email me, and I will let you know what I take. And thank you for your kind comment.
Dr. Ladd, I found this and stayed up past my bedtime to read the complete article. THANK YOU for your time in preparing this – it is informative, fact based, and I detected no “hype” so my anxiety level did not increase. I’ve shared it with others so they too can be a little less anxious in this situation. Your advice is always welcomed. Stay healthy.
Thank you Sharon. I appreciate your kind comments more than you know. Be well.
I read your discussion of Proglucamune and when you suggest not using it. I have Chronic Lymphocytic Leukemia (in remission at this time) and am wondering if it is best to avoid Proglucamune since it it increases the production of Lymphocytes. Don’t need more of the CLL Lymphocytes. Met you in the Dallas area a few years ago.
Walter, just for clarification for other readers, I did not mention any brand names or brand products. Regarding beta glucans, it helps fight cancer cells. If i had CLL, I would take at least 4, if not 6 tablets per day. It does not increase the production of lymphocytes. It modulates the immune system to function normally. This is not medical advice, but information only. Please read my complete medical disclaimer in the footer. Thank you.
Thanks. I did copy and paste the product name from and earlier post. I met you a meeting for the brand and was very impressed with you. Also, I have been wanting this information very much to help me in making a decision about using the product. Again, thanks very much